

Myocardial dysfunction after out-of-hospital cardiac arrest: predictors and prognostic implications
- PMID: 28983759
- PMCID: PMC5967989
- DOI: 10.1007/s11739-017-1756-z
Myocardial dysfunction after out-of-hospital cardiac arrest: predictors and prognostic implications
Abstract
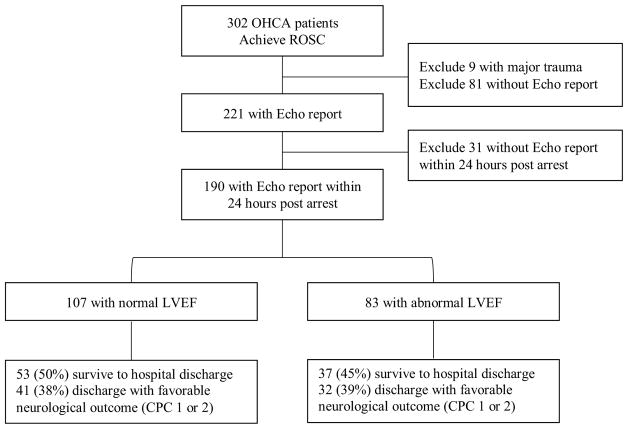
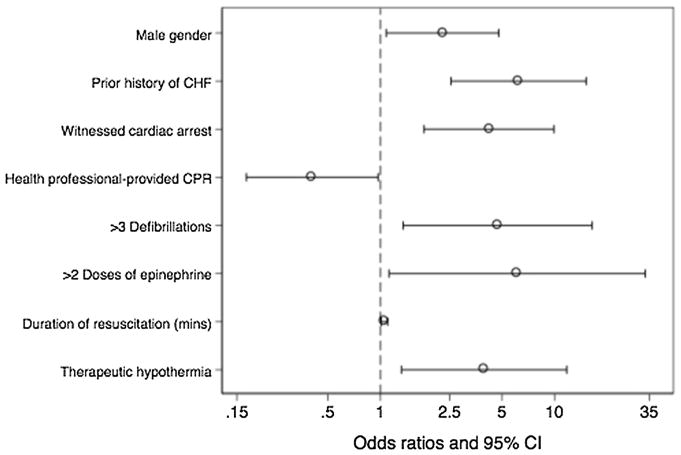
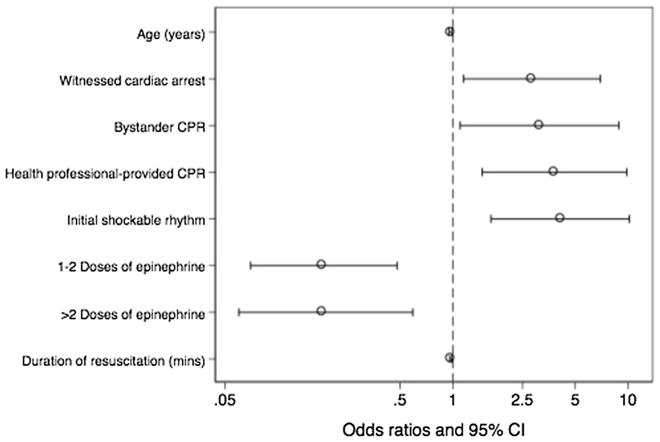
We aim to determine the incidence of early myocardial dysfunction after out-of-hospital cardiac arrest, risk factors associated with its development, and association with outcome. A retrospective chart review was performed among consecutive out-of-hospital cardiac arrest (OHCA) patients who underwent echocardiography within 24 h of return of spontaneous circulation at three urban teaching hospitals. Our primary outcome is early myocardial dysfunction, defined as a left ventricular ejection fraction < 40% on initial echocardiogram. We also determine risk factors associated with myocardial dysfunction using multivariate analysis, and examine its association with survival and neurologic outcome. A total of 190 patients achieved ROSC and underwent echocardiography within 24 h. Of these, 83 (44%) patients had myocardial dysfunction. A total of 37 (45%) patients with myocardial dysfunction survived to discharge, 39% with intact neurologic status. History of congestive heart failure (OR 6.21; 95% CI 2.54-15.19), male gender (OR 2.27; 95% CI 1.08-4.78), witnessed arrest (OR 4.20; 95% CI 1.78-9.93), more than three doses of epinephrine (OR 6.10; 95% CI 1.12-33.14), more than four defibrillations (OR 4.7; 95% CI 1.35-16.43), longer duration of resuscitation (OR 1.06; 95% CI 1.01-1.10), and therapeutic hypothermia (OR 3.93; 95% CI 1.32-11.75) were associated with myocardial dysfunction. Cardiopulmonary resuscitation immediately initiated by healthcare personnel was associated with lower odds of myocardial dysfunction (OR 0.40; 95% CI 0.17-0.97). There was no association between early myocardial dysfunction and mortality or neurological outcome. Nearly half of OHCA patients have myocardial dysfunction. A number of clinical factors are associated with myocardial dysfunction, and may aid providers in anticipating which patients need early diagnostic evaluation and specific treatments. Early myocardial dysfunction is not associated with neurologically intact survival.
Keywords: Cardiac arrest; Echocardiography; Myocardial dysfunction; Neurological outcome; Out-of-hospital.
Figures
References
-
- Nichol G, Rumsfeld J, Eigel B, et al. Essential features of designating out-of-hospital cardiac arrest as a reportable event: a scientific statement from the American Heart Association Emergency Cardiovascular Care Committee; Council on Cardiopulmonary, Perioperative, and Critical Care; Council on Cardiovascular Nursing; Council on Clinical Cardiology; and Quality of Care and Outcomes Research Interdisciplinary Working Group. Circulation. 2008;117(17):2299–2308. - PubMed
-
- Nolan JP, Neumar RW, Adrie C, et al. Post-cardiac arrest syndrome: epidemiology, pathophysiology, treatment, and prognostication. Resuscitation. 2008;79(3):350–379. - PubMed
-
- Laurent I, Monchi M, Chiche JD, et al. Reversible myocardial dysfunction in survivors of out-of-hospital cardiac arrest. J Am Coll Cardiol. 2002;40(12):2110–2116. - PubMed
-
- Ruiz-Bailen M, Aguayo de Hoyos E, Ruiz-Navarro S, et al. Reversible myocardial dysfunction after cardiopulmonary resuscitation. Resuscitation. 2005;66(2):175–181. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
