

Progressive Changes in Walking Kinematics and Kinetics After Anterior Cruciate Ligament Injury and Reconstruction: A Review and Meta-Analysis
- PMID: 28985125
- PMCID: PMC5634233
- DOI: 10.4085/1062-6050-52.6.06
Progressive Changes in Walking Kinematics and Kinetics After Anterior Cruciate Ligament Injury and Reconstruction: A Review and Meta-Analysis
Abstract
Context: Anterior cruciate ligament (ACL) injury and ACL reconstruction (ACLR) result in persistent alterations in lower extremity movement patterns. The progression of lower extremity biomechanics from the time of injury has not been described.
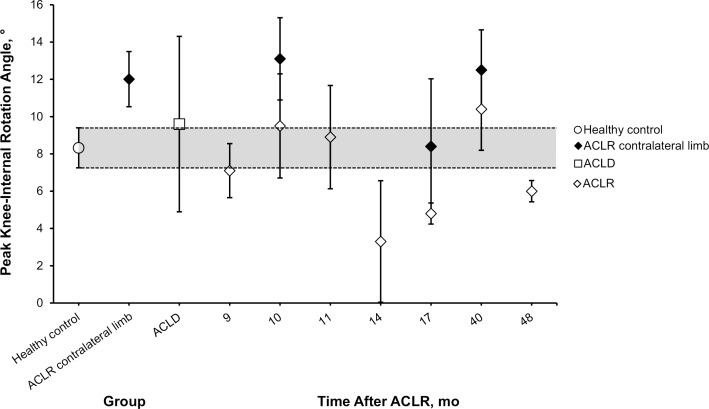
Objective: To compare the 3-dimensional (3D) lower extremity kinematics and kinetics of walking among individuals with ACL deficiency (ACLD), individuals with ACLR, and healthy control participants from 3 to 64 months after ACLR.
Data sources: We searched PubMed and Web of Science from 1970 through 2013.
Study selection and data extraction: We selected only articles that provided peak kinematic and kinetic values during walking in individuals with ACLD or ACLR and comparison with a healthy control group or the contralateral uninjured limb.
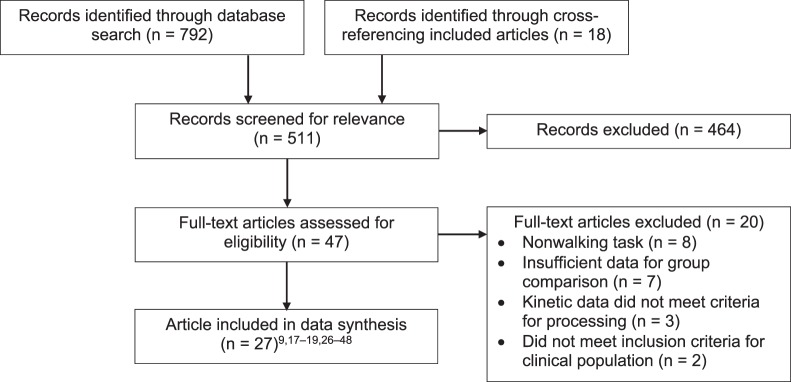
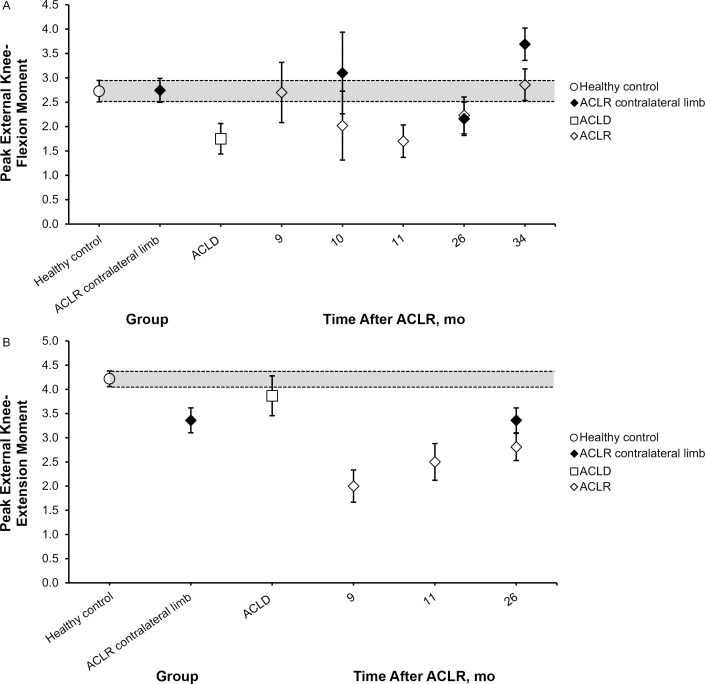
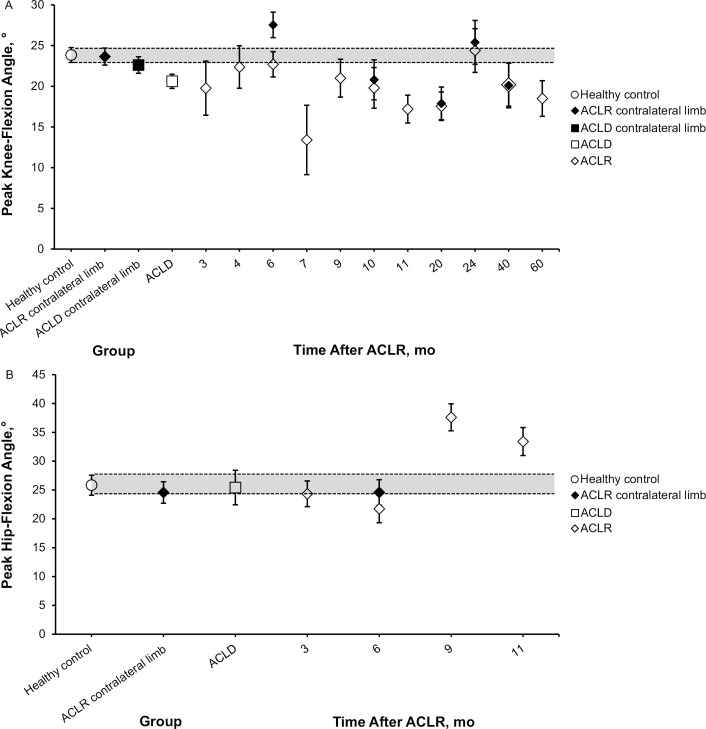
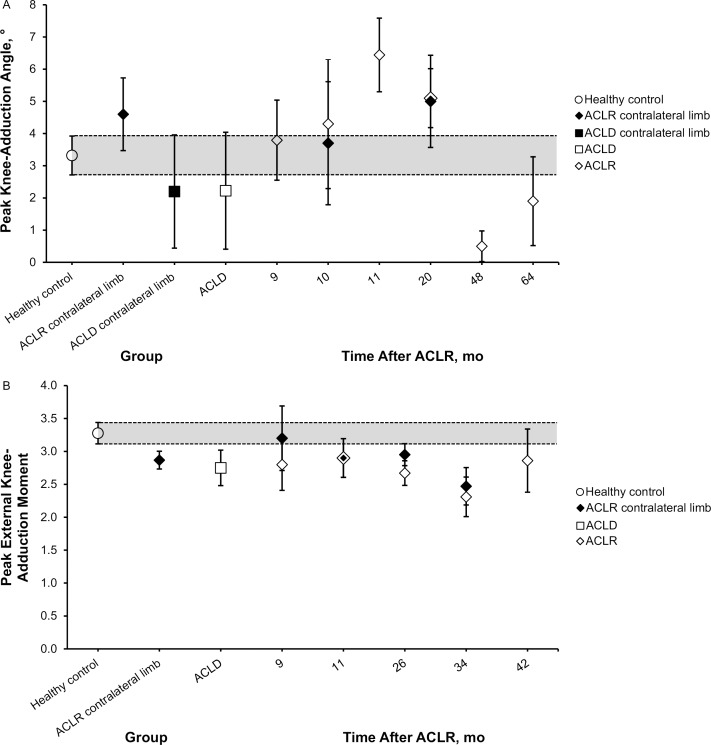
Data synthesis: A total of 27 of 511 identified studies were included. Weighted means, pooled standard deviations, and 95% confidence intervals were calculated for the healthy control, ACLD, and ACLR groups at each reported time since surgery. The magnitude of between-groups (ACLR versus ACLD, control, or contralateral limb) differences at each time point was evaluated using Cohen d effect sizes and associated 95% confidence intervals. Peak knee-flexion angle (Cohen d = -0.41) and external knee-extensor moment (Cohen d = -0.68) were smaller in the ACLD than in the healthy control group. Peak knee-flexion angle (Cohen d range = -0.78 to -1.23) and external knee-extensor moment (Cohen d range = -1.39 to -2.16) were smaller in the ACLR group from 10 to 40 months after ACLR. Reductions in external knee-adduction moment (Cohen d range = -0.50 to -1.23) were present from 9 to 42 months after ACLR.
Conclusions: Reductions in peak knee-flexion angle, external knee-flexion moment, and external knee-adduction moment were present in the ACLD and ACLR groups. This movement profile during the loading phase of gait has been linked to knee-cartilage degeneration and may contribute to the development of osteoarthritis after ACLR.
Keywords: anterior cruciate ligament deficiency; gait biomechanics; knee osteoarthritis; movement dysfunction.
Figures
References
-
- Mall NA, Chalmers PN, Moric M, et al. Incidence and trends of anterior cruciate ligament reconstruction in the United States. Am J Sports Med. 2014; 42 10: 2363– 2370. - PubMed
-
- Ardern CL, Webster KE, Taylor NF, Feller JA. . Return to sport following anterior cruciate ligament reconstruction surgery: a systematic review and meta-analysis of the state of play. Br J Sports Med. 2011; 45 7: 596– 606. - PubMed
-
- Oiestad BE, Holm I, Engebretsen L, Risberg MA. . The association between radiographic knee osteoarthritis and knee symptoms, function and quality of life 10−15 years after anterior cruciate ligament reconstruction. Br J Sports Med. 2011; 45 7: 583– 588. - PubMed
-
- Ardern CL, Webster KE, Taylor NF, Feller JA. . Return to the preinjury level of competitive sport after anterior cruciate ligament reconstruction surgery: two-thirds of patients have not returned by 12 months after surgery. Am J Sports Med. 2011; 39 3: 538– 543. - PubMed
-
- Otzel DM, Chow JW, Tillman MD. . Long-term deficits in quadriceps strength and activation following anterior cruciate ligament reconstruction. Phys Ther Sport. 2015; 16 1: 22– 28. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
