

"Good things come in small packages": application of exosome-based therapeutics in neonatal lung injury
- PMID: 28985201
- PMCID: PMC5876073
- DOI: 10.1038/pr.2017.256
"Good things come in small packages": application of exosome-based therapeutics in neonatal lung injury
Abstract
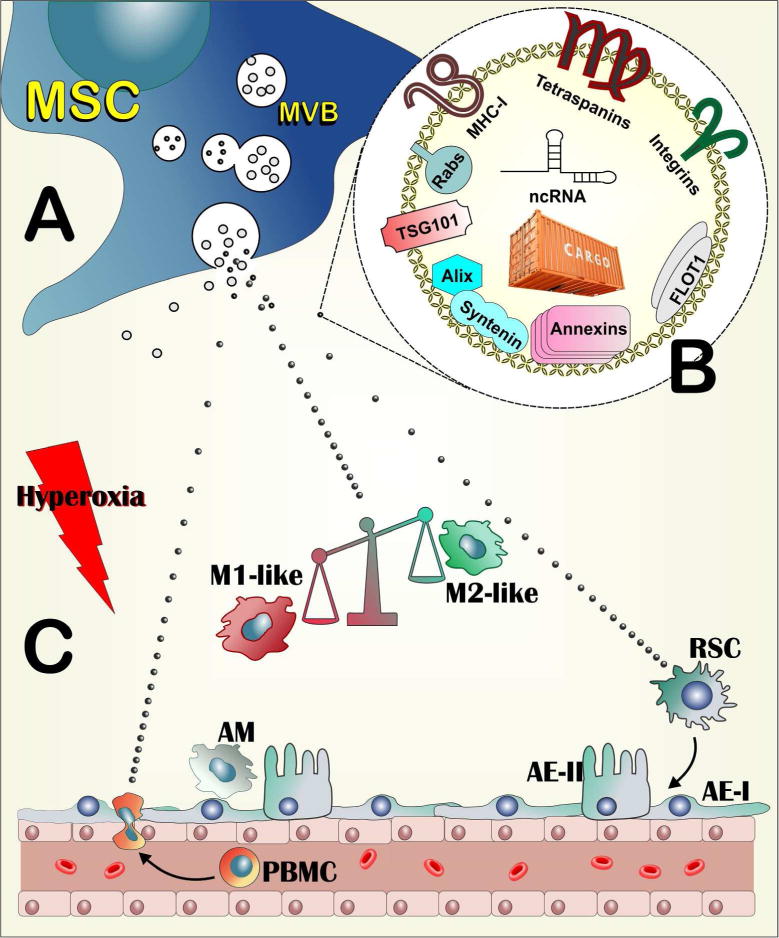
Infants born at very low gestational age contribute disproportionately to neonatal morbidity and mortality. Advancements in antenatal steroid therapies and surfactant replacement have favored the survival of infants with ever-more immature lungs. Despite such advances in medical care, cardiopulmonary and neurological impairment prevail in constituting the major adverse outcomes for neonatal intensive care unit survivors. With no single effective therapy for either the prevention or treatment of such neonatal disorders, the need for new tools to treat and reduce risk of further complications associated with extreme preterm birth is urgent. Mesenchymal stem/stromal cell (MSC)-based approaches have shown promise in numerous experimental models of lung injury relevant to neonatology. Recent studies have highlighted that the therapeutic potential of MSCs is harnessed in their secretome, and that the therapeutic vector therein is represented by the exosomes released by MSCs. In this review, we summarize the development and significance of stem cell-based therapies for neonatal diseases, focusing on preclinical models of neonatal lung injury. We emphasize the development of MSC exosome-based therapeutics and comment on the challenges in bringing these promising interventions to clinic.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
