

Safety and immunogenicity of rVSVΔG-ZEBOV-GP Ebola vaccine in adults and children in Lambaréné, Gabon: A phase I randomised trial
- PMID: 28985239
- PMCID: PMC5630143
- DOI: 10.1371/journal.pmed.1002402
Safety and immunogenicity of rVSVΔG-ZEBOV-GP Ebola vaccine in adults and children in Lambaréné, Gabon: A phase I randomised trial
Abstract
Background: The rVSVΔG-ZEBOV-GP vaccine prevented Ebola virus disease when used at 2 × 107 plaque-forming units (PFU) in a trial in Guinea. This study provides further safety and immunogenicity data.
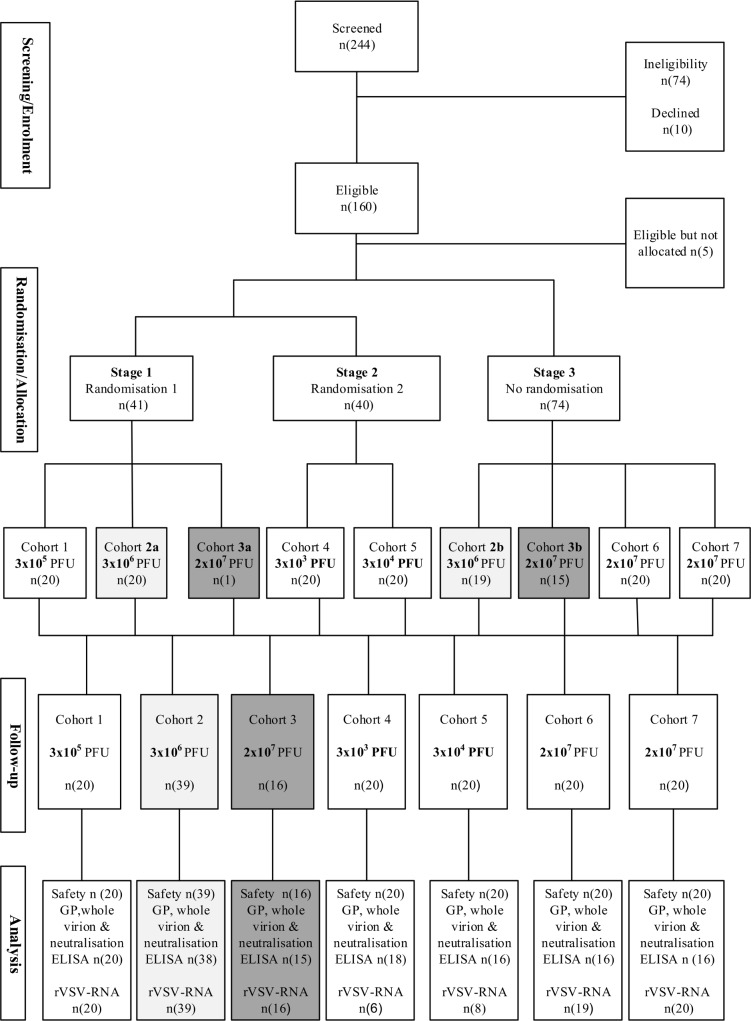
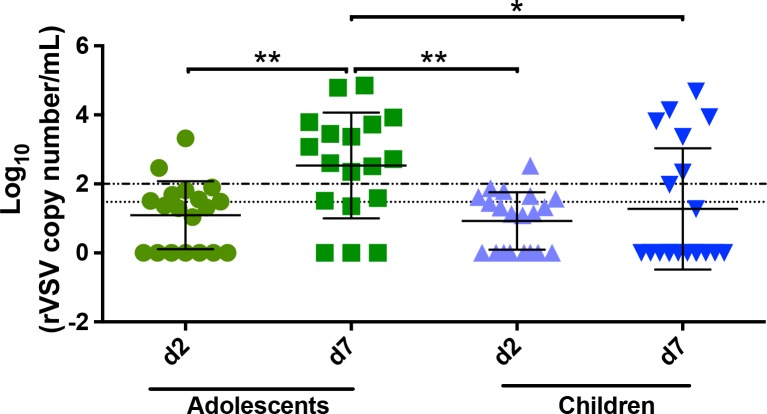
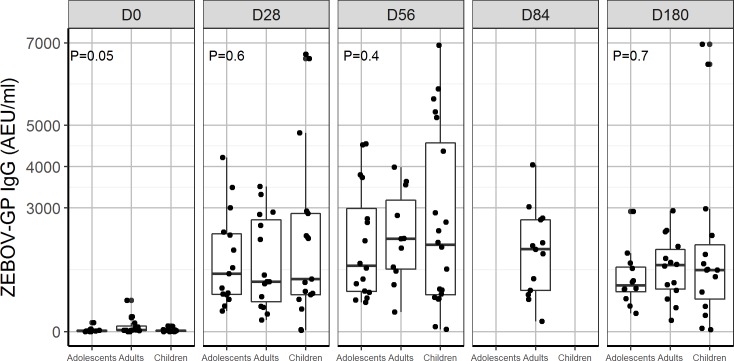
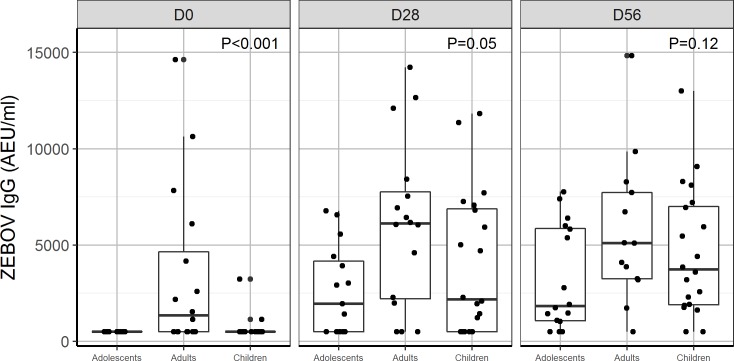
Methods and findings: A randomised, open-label phase I trial in Lambaréné, Gabon, studied 5 single intramuscular vaccine doses of 3 × 103, 3 × 104, 3 × 105, 3 × 106, or 2 × 107 PFU in 115 adults and a dose of 2 × 107 PFU in 20 adolescents and 20 children. The primary objective was safety and tolerability 28 days post-injection. Immunogenicity, viraemia, and shedding post-vaccination were evaluated as secondary objectives. In adults, mild-to-moderate adverse events were frequent, but there were no serious or severe adverse events related to vaccination. Before vaccination, Zaire Ebola virus (ZEBOV)-glycoprotein (GP)-specific and ZEBOV antibodies were detected in 11% and 27% of adults, respectively. In adults, 74%-100% of individuals who received a dose 3 × 104, 3 × 105, 3 × 106, or 2 × 107 PFU had a ≥4.0-fold increase in geometric mean titres (GMTs) of ZEBOV-GP-specific antibodies at day 28, reaching GMTs of 489 (95% CI: 264-908), 556 (95% CI: 280-1,101), 1,245 (95% CI: 899-1,724), and 1,503 (95% CI: 931-2,426), respectively. Twenty-two percent of adults had a ≥4-fold increase of ZEBOV antibodies, with GMTs at day 28 of 1,015 (647-1,591), 1,887 (1,154-3,085), 1,445 (1,013-2,062), and 3,958 (2,249-6,967) for the same doses, respectively. These antibodies persisted up to day 180 for doses ≥3 × 105 PFU. Adults with antibodies before vaccination had higher GMTs throughout. Neutralising antibodies were detected in more than 50% of participants at doses ≥3 × 105 PFU. As in adults, no serious or severe adverse events related to vaccine occurred in adolescents or children. At day 2, vaccine RNA titres were higher for adolescents and children than adults. At day 7, 78% of adolescents and 35% of children had recombinant vesicular stomatitis virus RNA detectable in saliva. The vaccine induced high GMTs of ZEBOV-GP-specific antibodies at day 28 in adolescents, 1,428 (95% CI: 1,025-1,989), and children, 1,620 (95% CI: 806-3,259), and in both groups antibody titres increased up to day 180. The absence of a control group, lack of stratification for baseline antibody status, and imbalances in male/female ratio are the main limitations of this study.
Conclusions: Our data confirm the acceptable safety and immunogenicity profile of the 2 × 107 PFU dose in adults and support consideration of lower doses for paediatric populations and those who request boosting.
Trial registration: Pan African Clinical Trials Registry PACTR201411000919191.
Conflict of interest statement
The authors of this manuscript have the following competing interests: VM and MK, representing the WHO, declare partial support for the study from the Wellcome Trust and the Bill and Melinda Gates Foundation. Declare no further conflict of interest. SK is a member of the Editorial Board of PLOS Medicine. There are no further potential conflicts of interests to declare.
Figures
References
-
- World Health Organization Regional Office for Africa. WHO declares the end of the most recent Ebola virus disease outbreak in Liberia. Brazzaville (Republic of the Congo): World Health Organization Regional Office for Africa; 2016. June 9 [cited 2017 Sep 12]. Available from: http://www.afro.who.int/news/who-declares-end-most-recent-ebola-virus-di....
-
- World Health Organization. Ebola situation report—30 March 2016. Geneva: World Health Organization; 2016 [cited 2016 Apr 29]. Available from: http://apps.who.int/ebola/current-situation/ebola-situation-report-30-ma....
-
- World Health Organization. Ebola outbreak 2014–2015. Geneva: World Health Organization; 2016. [cited 2017 Mar 1]. Available from: http://who.int/csr/disease/ebola/en/.
-
- Sridhar S. Clinical development of Ebola vaccines. Ther Adv vaccines. 2015;3(5–6):125–38. doi: 10.1177/2051013615611017 - DOI - PMC - PubMed
-
- Wang Y, Li J, Hu Y, Liang Q, Wei M, Zhu F. Ebola vaccines in clinical trial: the promising candidates. Hum Vaccin Immunother. 2017;13(1):153–68. doi: 10.1080/21645515.2016.1225637 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
