

Improving admission medication reconciliation with pharmacists or pharmacy technicians in the emergency department: a randomised controlled trial
- PMID: 28986515
- PMCID: PMC5912995
- DOI: 10.1136/bmjqs-2017-006761
Improving admission medication reconciliation with pharmacists or pharmacy technicians in the emergency department: a randomised controlled trial
Abstract
Background: Admission medication history (AMH) errors frequently cause medication order errors and patient harm.
Objective: To quantify AMH error reduction achieved when pharmacy staff obtain AMHs before admission medication orders (AMO) are placed.
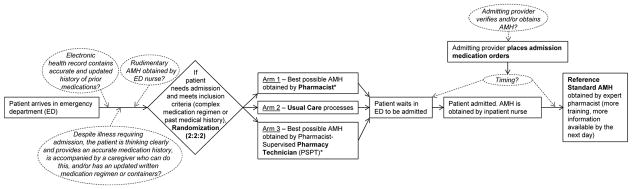
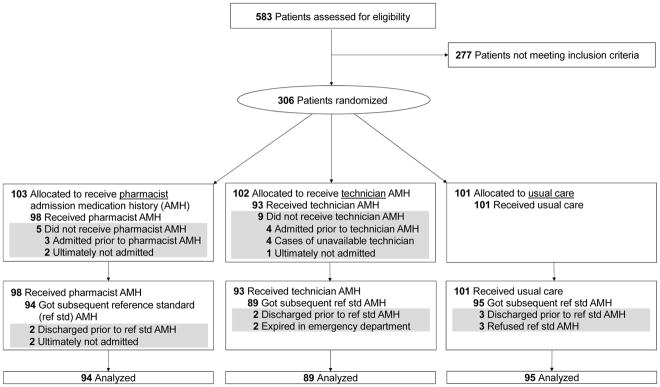
Methods: This was a three-arm randomised controlled trial of 306 inpatients. In one intervention arm, pharmacists, and in the second intervention arm, pharmacy technicians, obtained initial AMHs prior to admission. They obtained and reconciled medication information from multiple sources. All arms, including the control arm, received usual AMH care, which included variation in several common processes. The primary outcome was severity-weighted mean AMH error score. To detect AMH errors, all patients received reference standard AMHs, which were compared with intervention and control group AMHs. AMH errors and resultant AMO errors were independently identified and rated by ≥2 investigators as significant, serious or life threatening. Each error was assigned 1, 4 or 9 points, respectively, to calculate severity-weighted AMH and AMO error scores for each patient.
Results: Patient characteristics were similar across arms (mean±SD age 72±16 years, number of medications 15±7). Analysis was limited to 278 patients (91%) with reference standard AMHs. Mean±SD AMH errors per patient in the usual care, pharmacist and technician arms were 8.0±5.6, 1.4±1.9 and 1.5±2.1, respectively (p<0.0001). Mean±SD severity-weighted AMH error scores were 23.0±16.1, 4.1±6.8 and 4.1±7.0 per patient, respectively (p<0.0001). These AMH errors led to a mean±SD of 3.2±2.9, 0.6±1.1 and 0.6±1.1 AMO errors per patient, and mean severity-weighted AMO error scores of 6.9±7.2, 1.5±2.9 and 1.2±2.5 per patient, respectively (both p<0.0001).
Conclusions: Pharmacists and technicians reduced AMH errors and resultant AMO errors by over 80%. Future research should examine other sites and patient-centred outcomes.
Trial registration number: NCT02026453.
Keywords: health services research; healthcare quality improvement; human error; medication reconciliation; pharmacists.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: JP currently receives funding from the American Society for Health-System Pharmacists Research and Education Foundation to design a toolkit for pharmacists to use in postdischarge medication management.
Figures
References
-
- Bates DW, Cullen DJ, Laird N, et al. Incidence of adverse drug events and potential adverse drug events. Implications for prevention. ADE Prevention Study Group. Jama. 1995;274(1):29–34. - PubMed
-
- Aspden PWJ, Bootman JL, Cronenwett LR. Preventing Medication Errors: Quality Chasm Series. Washington, DC: The National Academic Press; 2007.
-
- Cornish PL, Knowles SR, Marchesano R, Tam V, Shadowitz S, Juurlink DN, et al. Unintended medication discrepancies at the time of hospital admission. Archives of internal medicine. 2005;165(4):424–9. - PubMed
-
- Gleason KM, McDaniel MR, Feinglass J, Baker DW, Lindquist L, Liss D, et al. Results of the Medications at Transitions and Clinical Handoffs (MATCH) study: an analysis of medication reconciliation errors and risk factors at hospital admission. Journal of general internal medicine. 2010;25(5):441–7. - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical