

Effect of inspiratory synchronization during pressure-controlled ventilation on lung distension and inspiratory effort
- PMID: 28986852
- PMCID: PMC5630544
- DOI: 10.1186/s13613-017-0324-z
Effect of inspiratory synchronization during pressure-controlled ventilation on lung distension and inspiratory effort
Abstract
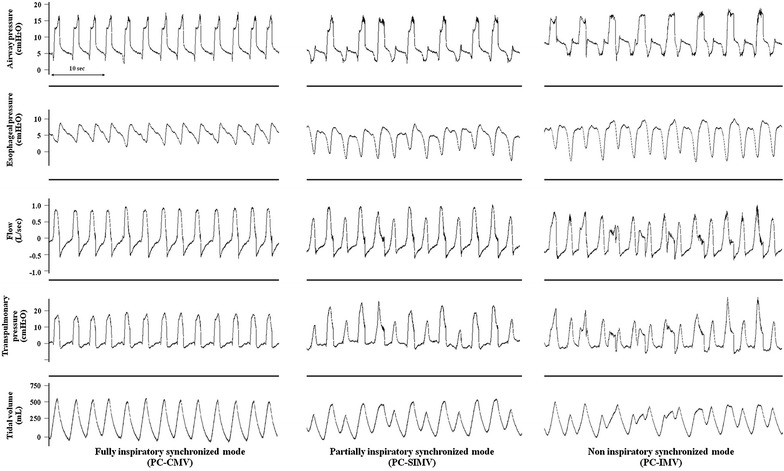
Background: In pressure-controlled (PC) ventilation, tidal volume (V T) and transpulmonary pressure (P L ) result from the addition of ventilator pressure and the patient's inspiratory effort. PC modes can be classified into fully, partially, and non-synchronized modes, and the degree of synchronization may result in different V T and P L despite identical ventilator settings. This study assessed the effects of three PC modes on V T, P L , inspiratory effort (esophageal pressure-time product, PTPes), and airway occlusion pressure, P 0.1. We also assessed whether P 0.1 can be used for evaluating patient effort.
Methods: Prospective, randomized, crossover physiologic study performed in 14 spontaneously breathing mechanically ventilated patients recovering from acute respiratory failure (1 subsequently withdrew). PC modes were fully (PC-CMV), partially (PC-SIMV), and non-synchronized (PC-IMV using airway pressure release ventilation) and were applied randomly; driving pressure, inspiratory time, and set respiratory rate being similar for all modes. Airway, esophageal pressure, P 0.1, airflow, gas exchange, and hemodynamics were recorded.
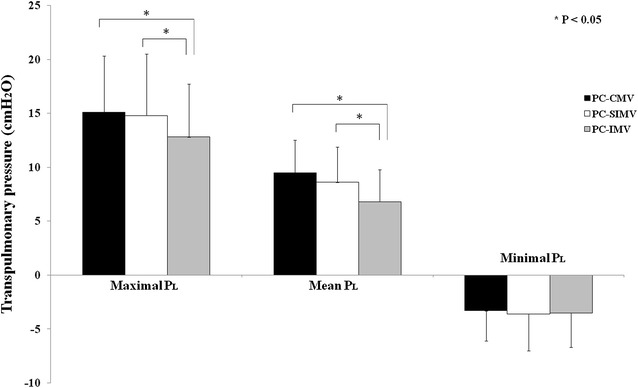
Results: V T was significantly lower during PC-IMV as compared with PC-SIMV and PC-CMV (387 ± 105 vs 458 ± 134 vs 482 ± 108 mL, respectively; p < 0.05). Maximal P L was also significantly lower (13.3 ± 4.9 vs 15.3 ± 5.7 vs 15.5 ± 5.2 cmH2O, respectively; p < 0.05), but PTPes was significantly higher in PC-IMV (215.6 ± 154.3 vs 150.0 ± 102.4 vs 130.9 ± 101.8 cmH2O × s × min-1, respectively; p < 0.05), with no differences in gas exchange and hemodynamic variables. PTPes increased by more than 15% in 10 patients and by more than 50% in 5 patients. An increased P 0.1 could identify high levels of PTPes.
Conclusions: Non-synchronized PC mode lowers V T and P L in comparison with more synchronized modes in spontaneously breathing patients but can increase patient effort and may need specific adjustments. Clinical Trial Registration Clinicaltrial.gov # NCT02071277.
Keywords: Airway pressure release ventilation; Lung-protective ventilation; Spontaneous ventilation; Transpulmonary pressure; Ventilator-induced lung injury.
Figures

References
-
- Putensen C, Mutz NJ, Putensen-Himmer G, Zinserling J. Spontaneous breathing during ventilatory support improves ventilation–perfusion distributions in patients with acute respiratory distress syndrome. Am J Respir Crit Care Med. 1999;159(4 Pt 1):1241–1248. doi: 10.1164/ajrccm.159.4.9806077. - DOI - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
