

Center practice drives variation in choice of US kidney transplant induction therapy: a retrospective analysis of contemporary practice
- PMID: 28987015
- PMCID: PMC5862637
- DOI: 10.1111/tri.13079
Center practice drives variation in choice of US kidney transplant induction therapy: a retrospective analysis of contemporary practice
Abstract
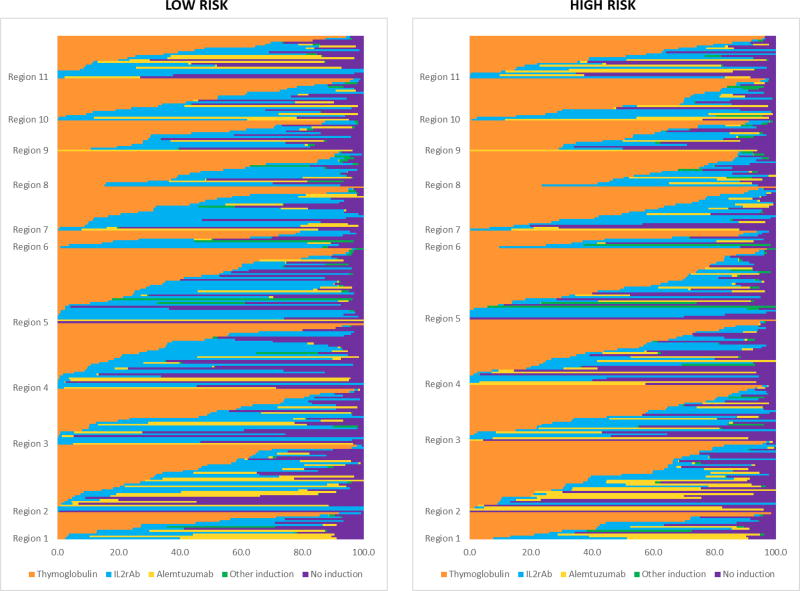
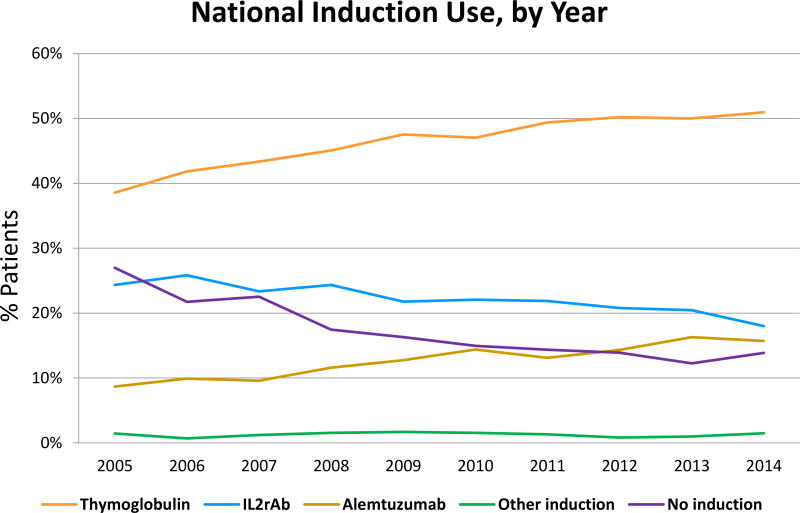
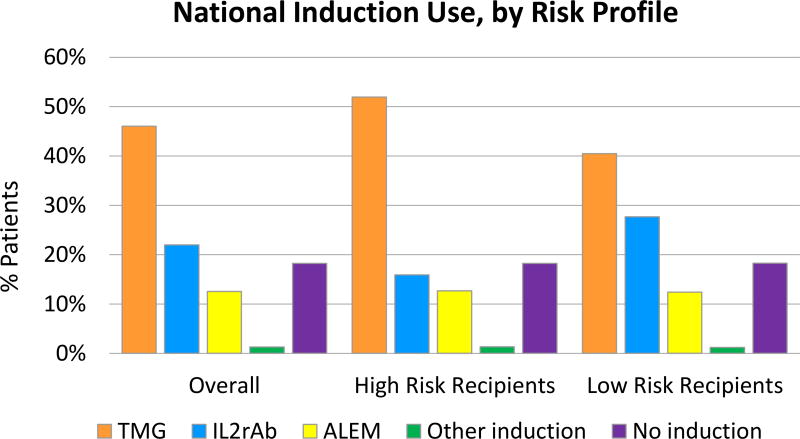
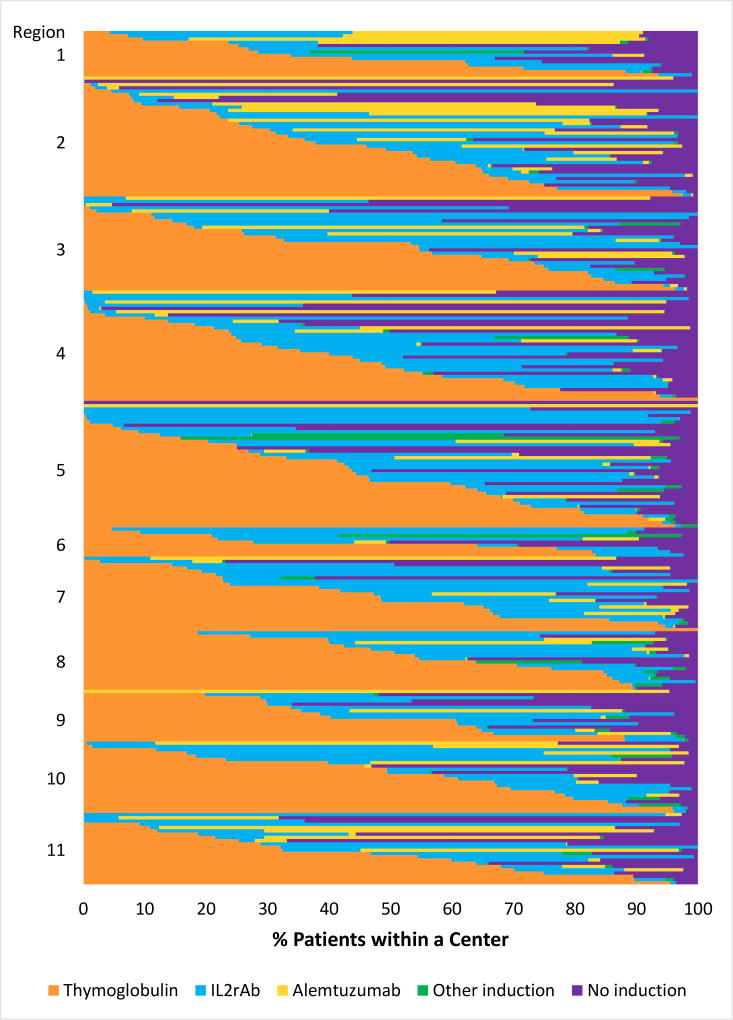
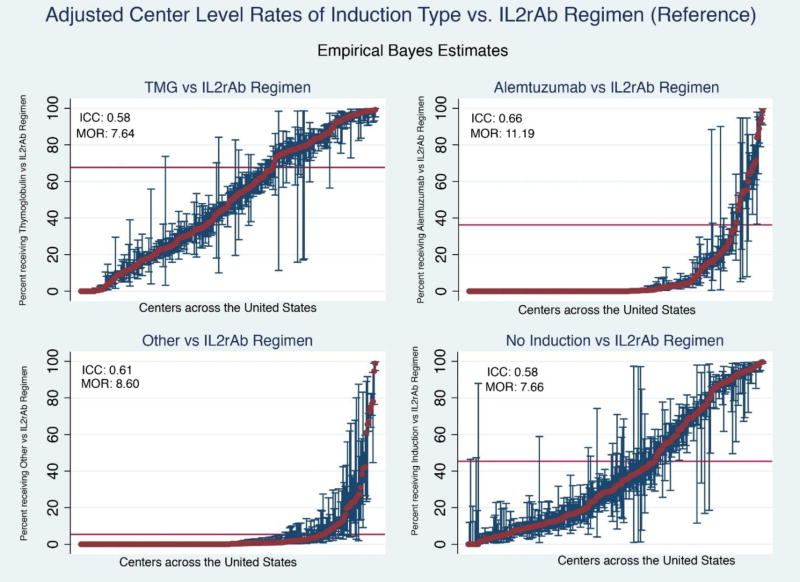
To assess factors that influence the choice of induction regimen in contemporary kidney transplantation, we examined center-identified, national transplant registry data for 166 776 US recipients (2005-2014). Bilevel hierarchical models were constructed, wherein use of each regimen was compared pairwise with use of interleukin-2 receptor blocking antibodies (IL2rAb). Overall, 82% of patients received induction, including thymoglobulin (TMG, 46%), IL2rAb (22%), alemtuzumab (ALEM, 13%), and other agents (1%). However, proportions of patients receiving induction varied widely across centers (0-100%). Recipients of living donor transplants and self-pay patients were less likely to receive induction treatment. Clinical factors associated with use of TMG or ALEM (vs. IL2rAb) included age, black race, sensitization, retransplant status, nonstandard deceased donor, and delayed graft function. However, these characteristics explained only 10-33% of observed variation. Based on intraclass correlation analysis, "center effect" explained most of the variation in TMG (58%), ALEM (66%), other (51%), and no induction (58%) use. Median odds ratios generated from case-factor adjusted models (7.66-11.19) also supported large differences in the likelihood of induction choices between centers. The wide variation in induction therapy choice across US transplant centers is not dominantly explained by differences in patient or donor characteristics; rather, it reflects center choice and practice.
Keywords: immunosuppression; induction; kidney transplantation; practice patterns.
© 2017 Steunstichting ESOT.
Conflict of interest statement
Figures
References
-
- Halloran PF. Immunosuppressive Drugs for Kidney Transplantation. New England Journal of Medicine. 2004;351(26):2715–29. - PubMed
-
- Charpentier B, Rostaing L, Berthoux F, Lang P, Civati G, Touraine JL, et al. A three-arm study comparing immediate tacrolimus therapy with antithymocyte globulin induction therapy followed by tacrolimus or cyclosporine A in adult renal transplant recipients. Transplantation. 2003;75(6):844–51. - PubMed
-
- Caillard S, Dharnidharka V, Agodoa L, Bohen E, Abbott K. Posttransplant lymphoproliferative disorders after renal transplantation in the United States in era of modern immunosuppression. Transplantation. 2005;80(9):1233–43. - PubMed
-
- Dharnidharka VR, Cherikh WS, Abbott KC. An OPTN analysis of national registry data on treatment of BK virus allograft nephropathy in the United States. Transplantation. 2009;87(7):1019–26. - PubMed
-
- Opelz G, Unterrainer C, Susal C, Dohler B. Efficacy and safety of antibody induction therapy in the current era of kidney transplantation. Nephrol Dial Transplant. 2016;31(10):1730–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
