

Outcomes of oxygen saturation targeting during delivery room stabilisation of preterm infants
- PMID: 28988158
- PMCID: PMC6490957
- DOI: 10.1136/archdischild-2016-312366
Outcomes of oxygen saturation targeting during delivery room stabilisation of preterm infants
Abstract
Objective: To determine the association between SpO2 at 5 min and preterm infant outcomes.
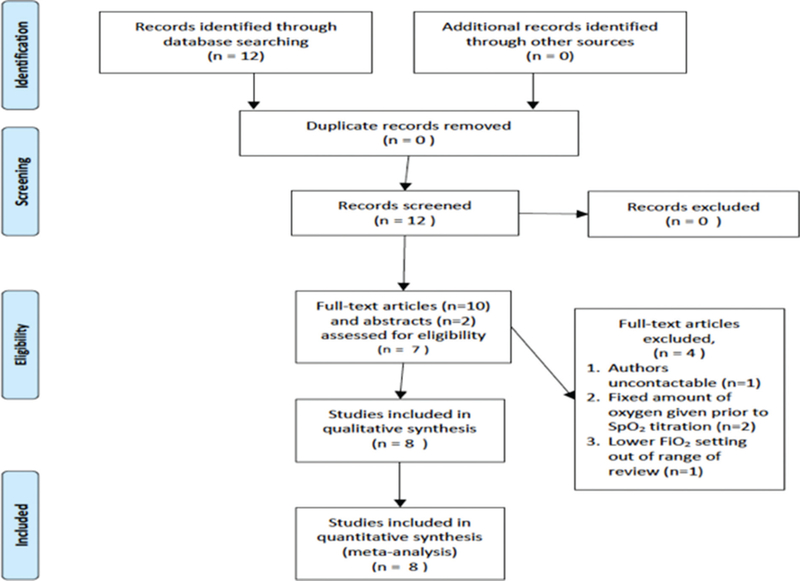
Design: Data from 768 infants <32 weeks gestation from 8 randomised controlled trials (RCTs) of lower (≤0.3) versus higher (≥0.6) initial inspiratory fractions of oxygen (FiO2) for resuscitation, were examined.
Setting: Individual patient analysis of 8 RCTs INTERVENTIONS: Lower (≤0.3) versus higher (≥0.6) oxygen resuscitation strategies targeted to specific predefined SpO2 before 10 min of age.
Patients: Infants <32 weeks gestation.
Main outcome measures: Relationship between SpO2 at 5 min, death and intraventricular haemorrhage (IVH) >grade 3.
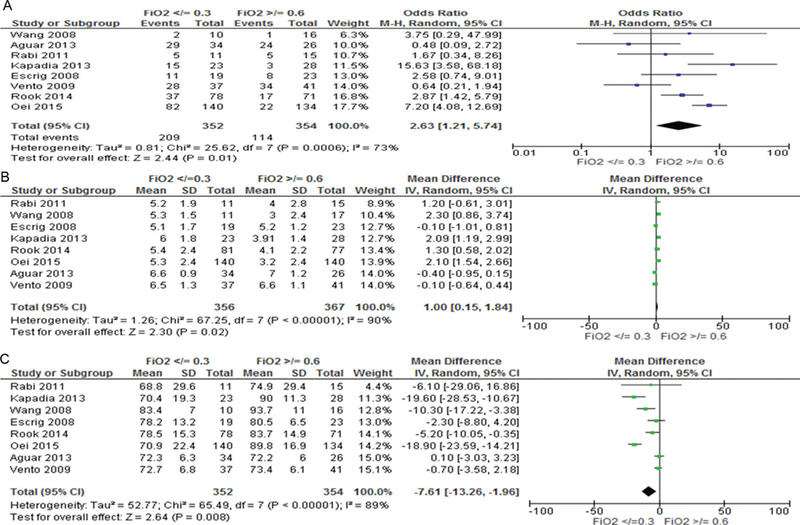
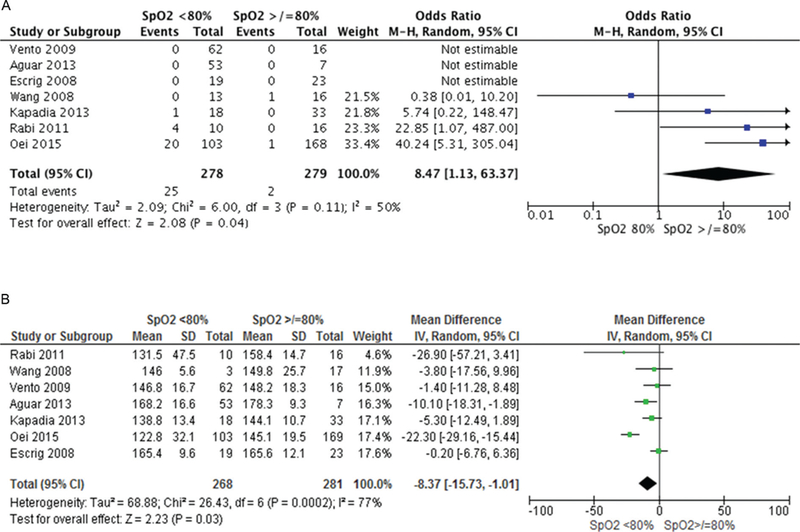
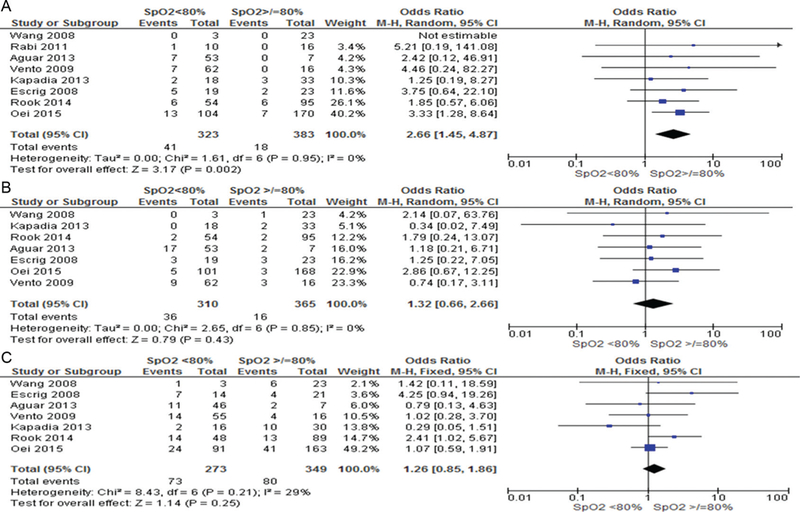
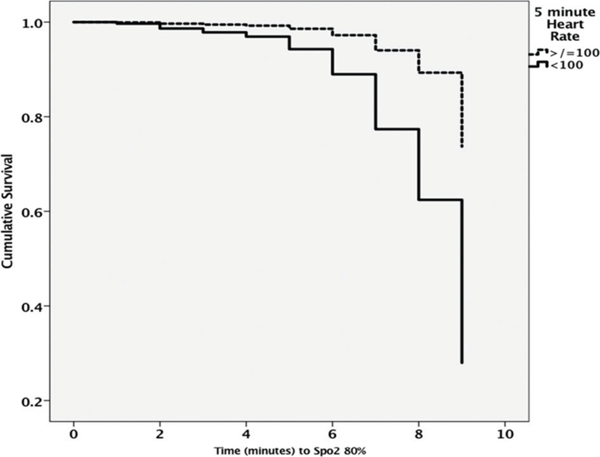
Results: 5 min SpO2 data were obtained from 706 (92%) infants. Only 159 (23%) infants met SpO2 study targets and 323 (46%) did not reach SpO280%. Pooled data showed decreased likelihood of reaching SpO280% if resuscitation was initiated with FiO2 <0.3 (OR 2.63, 95% CI 1.21 to 5.74, p<0.05). SpO2 <80% was associated with lower heart rates (mean difference -8.37, 95% CI -15.73 to -1.01, *p<0.05) and after accounting for confounders, with IVH (OR 2.04, 95% CI 1.01 to 4.11, p<0.05). Bradycardia (heart rate <100 bpm) at 5 min increased risk of death (OR 4.57, 95% CI 1.62 to 13.98, p<0.05). Taking into account confounders including gestation, birth weight and 5 min bradycardia, risk of death was significantly increased with time taken to reach SpO280%.
Conclusion: Not reaching SpO280% at 5 min is associated with adverse outcomes, including IVH. Whether this is because of infant illness or the amount of oxygen that is administered during stabilisation is uncertain and needs to be examined in randomised trials.
Keywords: neonatology; resuscitation.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Neonatal Resuscitation Program Part 13. Neonatal Resuscitation. https://eccguidelines.heart.org/wp-content/themes/eccstaging/dompdf-mast...
-
- Mariani G, Dik PB, Ezquer A, et al. Pre-ductal and post-ductal 02 saturation in healthy term neonates after birth. J Pediatr 2007;150:418–21. - PubMed
-
- Whyte SD, Sinha AK, Wyllie JP. Neonatal resuscitation-a practical assessment. Resuscitation 1999;40:21–5. - PubMed
-
- Clark R, Lui K, Oei J. The use of blended oxygen in the resuscitation of newborn infants in Australia and New Zealand - A suivey of current opinion and practice. J Paediatr Child Health 2009;45:31–5. - PubMed
-
- Ramji S, Ahuja S, Thirupuram S, et al. Resuscitation of asphyxic newborn infants with room air or 100% oxygen. Pediatr Res 1993;34:809–12. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous