

The oral microbiota in colorectal cancer is distinctive and predictive
- PMID: 28988196
- PMCID: PMC6204958
- DOI: 10.1136/gutjnl-2017-314814
The oral microbiota in colorectal cancer is distinctive and predictive
Abstract
Background and aims: Microbiota alterations are linked with colorectal cancer (CRC) and notably higher abundance of putative oral bacteria on colonic tumours. However, it is not known if colonic mucosa-associated taxa are indeed orally derived, if such cases are a distinct subset of patients or if the oral microbiome is generally suitable for screening for CRC.
Methods: We profiled the microbiota in oral swabs, colonic mucosae and stool from individuals with CRC (99 subjects), colorectal polyps (32) or controls (103).
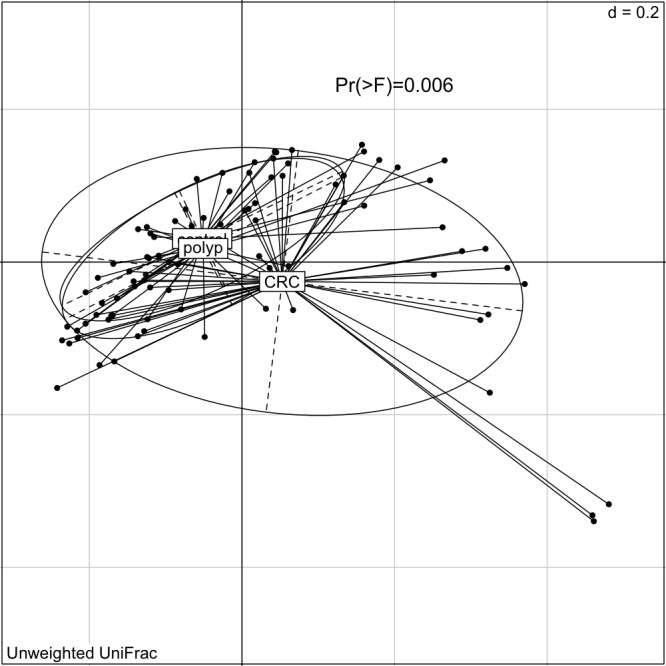
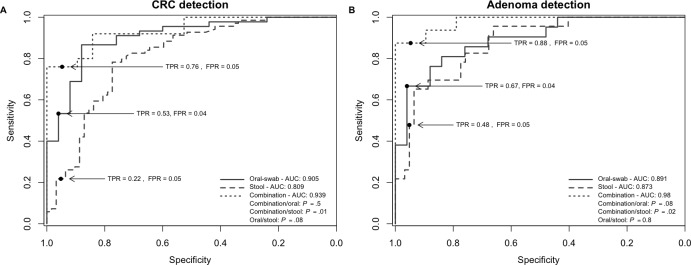
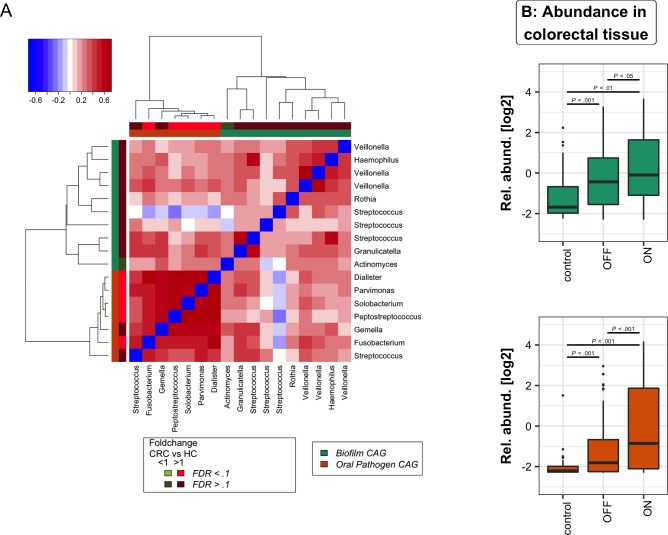
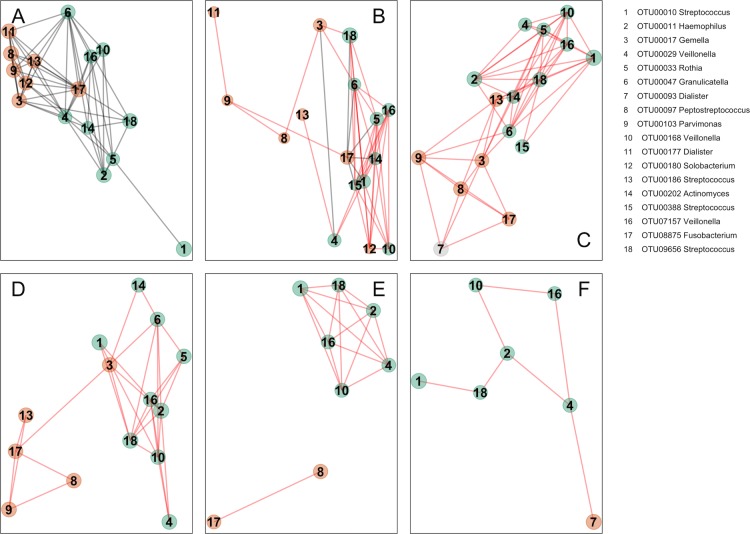
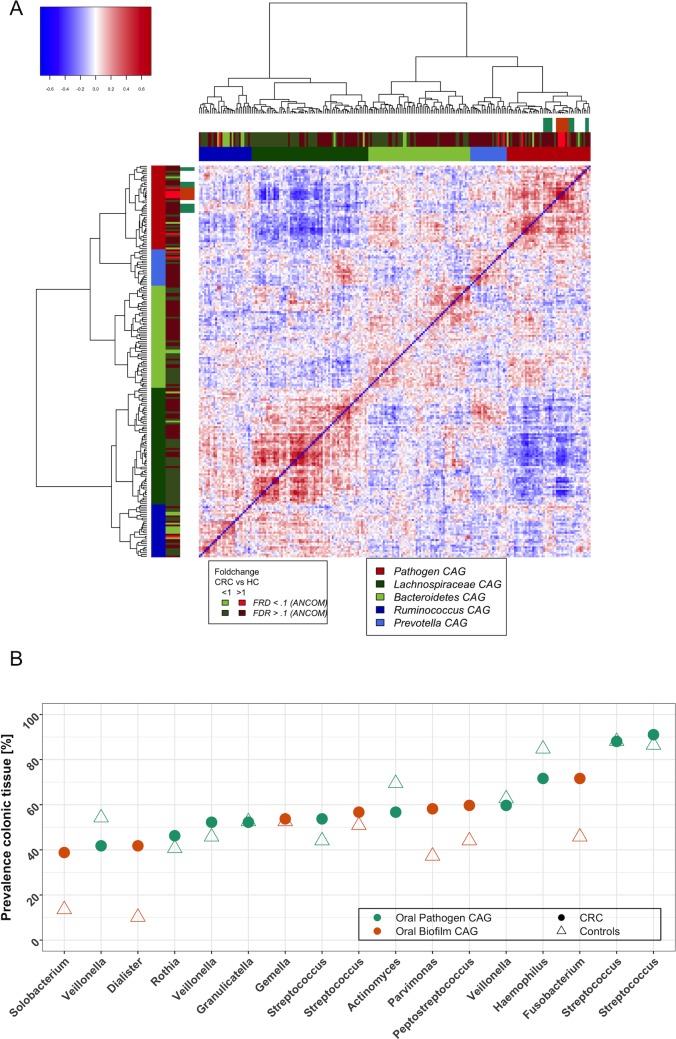
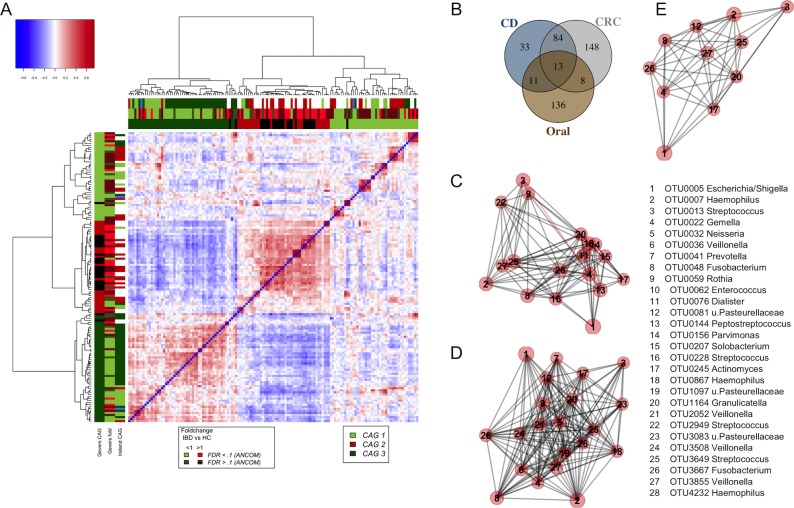
Results: Several oral taxa were differentially abundant in CRC compared with controls, for example, Streptococcus and Prevotellas pp. A classification model of oral swab microbiota distinguished individuals with CRC or polyps from controls (sensitivity: 53% (CRC)/67% (polyps); specificity: 96%). Combining the data from faecal microbiota and oral swab microbiota increased the sensitivity of this model to 76% (CRC)/88% (polyps). We detected similar bacterial networks in colonic microbiota and oral microbiota datasets comprising putative oral biofilm forming bacteria. While these taxa were more abundant in CRC, core networks between pathogenic, CRC-associated oral bacteria such as Peptostreptococcus, Parvimonas and Fusobacterium were also detected in healthy controls. High abundance of Lachnospiraceae was negatively associated with the colonisation of colonic tissue with oral-like bacterial networks suggesting a protective role for certain microbiota types against CRC, possibly by conferring colonisation resistance to CRC-associated oral taxa and possibly mediated through habitual diet.
Conclusion: The heterogeneity of CRC may relate to microbiota types that either predispose or provide resistance to the disease, and profiling the oral microbiome may offer an alternative screen for detecting CRC.
Keywords: colonic bacteria; colorectal cancer; colorectal cancer screening; diet; tumour markers.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Figures
Comment in
-
Gut microbiota: Oral microbiome could provide clues to CRC.Nat Rev Gastroenterol Hepatol. 2017 Dec;14(12):690. doi: 10.1038/nrgastro.2017.158. Epub 2017 Nov 2. Nat Rev Gastroenterol Hepatol. 2017. PMID: 29094724 No abstract available.
-
Patients with colorectal cancer have identical strains of Fusobacterium nucleatum in their colorectal cancer and oral cavity.Gut. 2019 Jul;68(7):1335-1337. doi: 10.1136/gutjnl-2018-316661. Epub 2018 Jun 22. Gut. 2019. PMID: 29934439 Free PMC article. No abstract available.
-
Time series analysis of microbiome and metabolome at multiple body sites in steady long-term isolation confinement.Gut. 2021 Jul;70(7):1409-1412. doi: 10.1136/gutjnl-2020-320666. Epub 2020 Sep 10. Gut. 2021. PMID: 32912857 No abstract available.
References
-
- Mf G, Smoot DT, pylori H. gastric malt lymphoma, and adenocarcinoma of the stomach. Semin Gastrointest Dis 2000;11:134–41 https://www.ncbi.nlm.nih.gov/pubmed/10950459 - PubMed
-
- Zeller G, Tap J, Voigt AY, et al. . Potential of fecal microbiota for early-stage detection of colorectal cancer. Mol Syst Biol 2014;10:766 doi:10.15252/msb.20145645 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous