

Epidemiology, diagnosis, and optimal management of glioma in adolescents and young adults
- PMID: 28989289
- PMCID: PMC5624597
- DOI: 10.2147/AHMT.S53391
Epidemiology, diagnosis, and optimal management of glioma in adolescents and young adults
Abstract
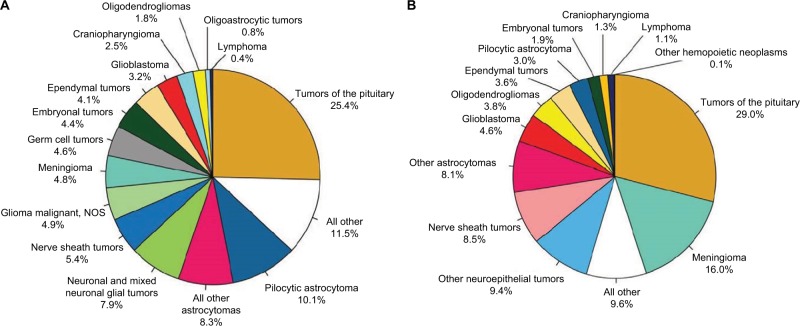
Neoplasms of the central nervous system (CNS) are the most frequently encountered solid tumors of childhood, but are less common in adolescents and young adults (AYA), aged 15-39 years. Gliomas account for 29%-35% of the CNS tumors in AYA, with approximately two-thirds being low-grade glioma (LGG) and the remaining being high-grade glioma (HGG). We review the epidemiology, work-up, and management of LGG and HGG, focusing on the particular issues faced by the AYA population relative to pediatric and adult populations. Visual pathway glioma and brainstem glioma, which represent unique clinical entities, are only briefly discussed. As a general management approach for both LGG and HGG, maximal safe resection should be attempted. AYA with LGG who undergo gross total resection (GTR) may be safely observed. As age increases and the risk factors for recurrence accumulate, adjuvant therapy should be more strongly considered with a strong consideration of advanced radiation techniques such as proton beam therapy to reduce long-term radiation-related toxicity. Recent results also suggest survival advantage for adult patients with the use of adjuvant chemotherapy when radiation is indicated. Whenever possible, AYA patients with HGG should be enrolled in a clinical trial for the benefit of centralized genetic and molecular prognostic review and best clinical care. Chemoradiation should be offered to all World Health Organization grade IV patients with concurrent and adjuvant chemotherapy after maximal safe resection. Younger adolescents with GTR of grade III lesions may consider radiotherapy alone or sequential radiotherapy and chemotherapy if unable to tolerate concurrent treatment. A more comprehensive classification of gliomas integrating pathology and molecular data is emerging, and this integrative strategy offers the potential to be more accurate and reproducible in guiding diagnostic, prognostic, and management decisions.
Keywords: adolescents; glioma; radiation; radiation therapy; young adults.
Conflict of interest statement
Disclosure The authors report no conflicts of interest in this work.
Figures
References
-
- National Cancer Institute at the National Institutes of Health Adolescents and young adults with cancer. [Accessed February 26, 2016]. Available from: http://www.cancer.gov/cancertopics/aya.
-
- Schwartzbaum JA, Fisher JL, Aldape KD, Wrensch M. Epidemiology and molecular pathology of glioma. Nat Clin Pract Neurol. 2006;2(9):494–503. - PubMed
-
- Unal E, Koksal Y, Cimen O, Paksoy Y, Tavli L. Malignant glioblastomatous transformation of a low-grade glioma in a child. Childs Nerv Syst. 2008;24(12):1385–1389. - PubMed
-
- Strong JA, Hatten HP, Jr, Brown MT, et al. Pilocytic astrocytoma: correlation between the initial imaging features and clinical aggressiveness. AJR Am J Roentgenol. 1993;161(2):369–372. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
