

Frontline Therapy for Classical Hodgkin Lymphoma by Stage and Prognostic Factors
- PMID: 28989291
- PMCID: PMC5624347
- DOI: 10.1177/1179554917731072
Frontline Therapy for Classical Hodgkin Lymphoma by Stage and Prognostic Factors
Abstract
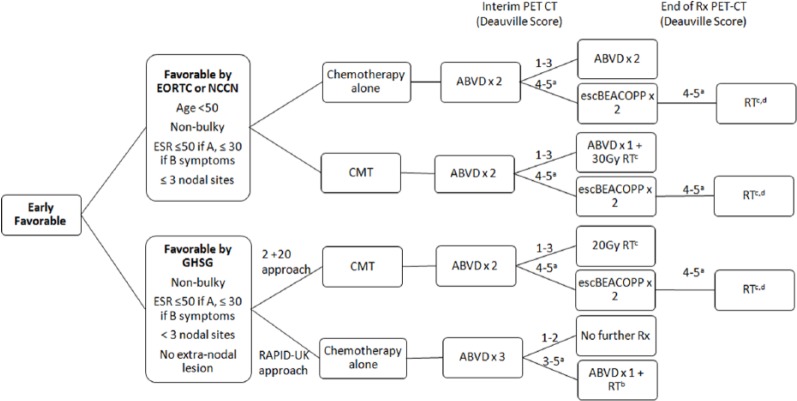
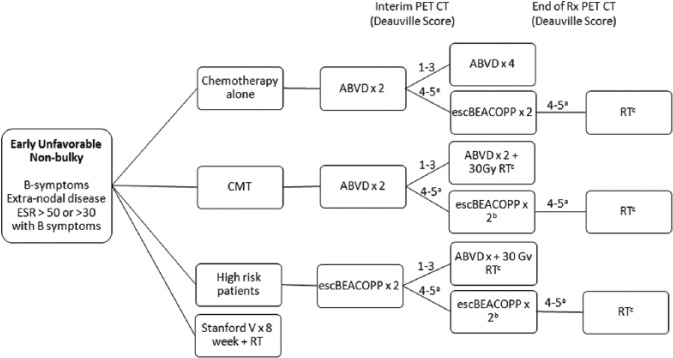
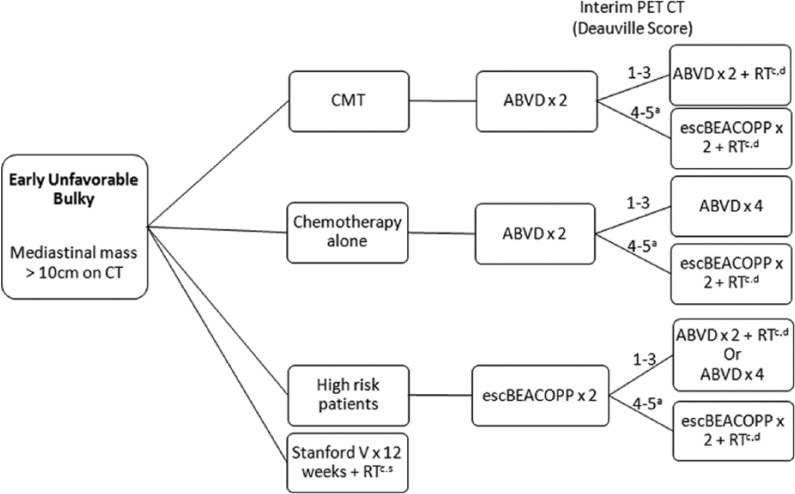
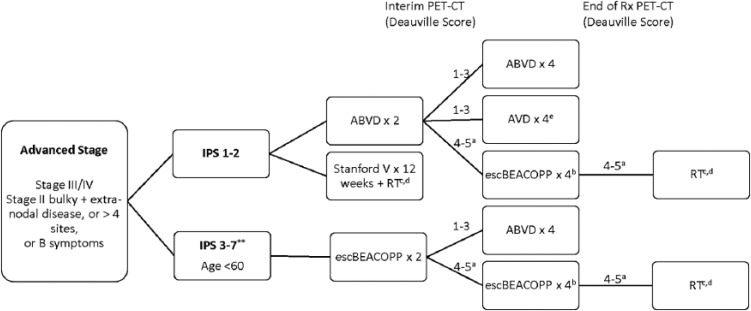
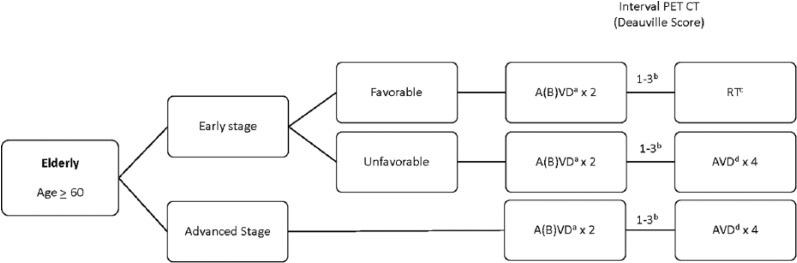
Hodgkin lymphoma is a highly curable malignancy in early and advanced stages. Most patients are diagnosed in their teens or twenties and are expected to live decades beyond their treatment. Therefore, the toxicity of treatment must be balanced with the goal of cure. Thus, treatment has been refined through prognostic models and positron emission tomography-computed tomography (PET-CT)-directed therapy. Stratification by prognostic models defines groups of patients with favorable characteristics who may be treated with less intensive therapy upfront, including fewer cycles of chemotherapy, lower doses of radiation, or omission of radiation altogether. Alternatively, high-risk patients may be assigned to a more aggressive initial approach. The modern use of interim PET-CT allows further tailoring of treatment by response.
Keywords: Hodgkin lymphoma; PET directed; advanced stage; early favorable; early unfavorable; prognosis.
Conflict of interest statement
Declaration of conflicting interests:The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Hasenclever D, Diehl V. A prognostic score for advanced Hodgkin’s disease. International Prognostic Factors Project on Advanced Hodgkin’s Disease. N Engl J Med. 1998;339:1506–1514. - PubMed
-
- Rigacci L, Puccini B, Zinzani PL, et al. The prognostic value of positron emission tomography performed after two courses (INTERIM-PET) of standard therapy on treatment outcome in early stage Hodgkin lymphoma: a multicentric study by the fondazione italiana linfomi (FIL). Am J Hematol. 2015;90:499–503. - PubMed
-
- Gallamini A, Patti C, Viviani S, et al. Early chemotherapy intensification with BEACOPP in advanced-stage Hodgkin lymphoma patients with a interim-PET positive after two ABVD courses. Br J Haematol. 2011;152:551–560. - PubMed
-
- Zinzani PL, Broccoli A, Gioia DM, et al. Interim positron emission tomography response-adapted therapy in advanced-stage Hodgkin lymphoma: final results of the phase II part of the HD0801 study. J Clin Oncol. 2016;34:1376–1385. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
