

Magnetic Resonance Imaging of Primary Hepatic Malignancies in Patients With and Without Chronic Liver Disease: A Pictorial Review
- PMID: 28989828
- PMCID: PMC5628780
- DOI: 10.7759/cureus.1539
Magnetic Resonance Imaging of Primary Hepatic Malignancies in Patients With and Without Chronic Liver Disease: A Pictorial Review
Abstract
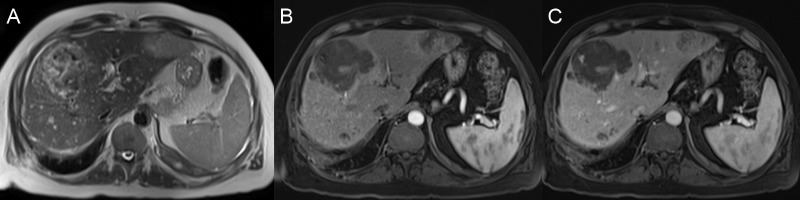
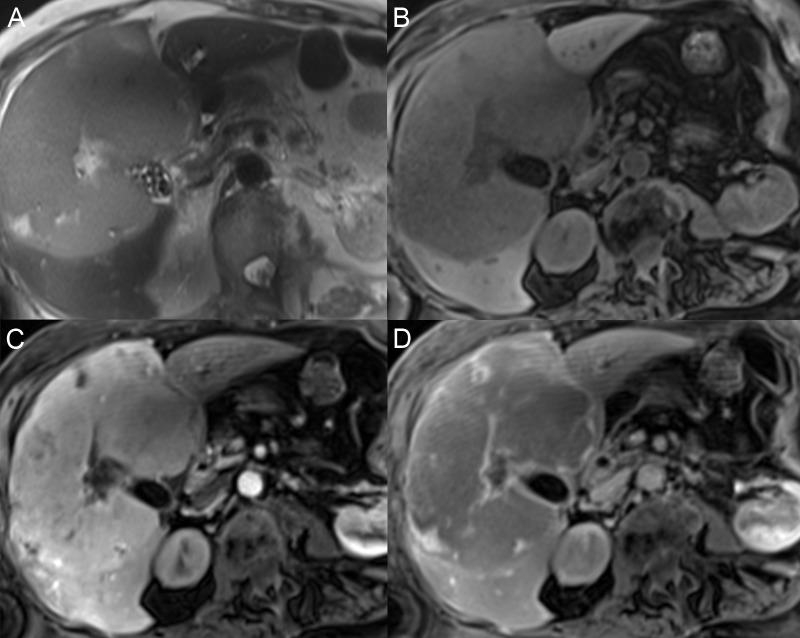
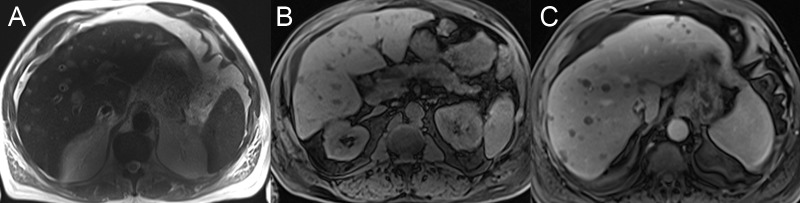
Primary hepatic malignancies are less common than metastatic diseases, but a recognition of these lesions is important for diagnosis and treatment planning. Magnetic resonance imaging (MRI) provides the most imaging information to diagnose lesions noninvasively and to narrow differential diagnoses. This paper reviews the imaging findings of chronic liver disease and primary hepatic malignancies, including hepatocellular carcinoma (HCC), intrahepatic cholangiocarcinoma (CCA), epithelioid hemangioendothelioma, hepatic angiosarcoma, and primary hepatic lymphoma. Clinical and MRI features are reviewed to improve the readers' recognition of these tumors, allowing for a narrower differential diagnosis when liver masses are encountered on abdominal imaging.
Keywords: bile duct neoplasms; carcinoma; cholangiocarcinoma; epithelioid; hemangioendothelioma; hemangiosarcoma; hepatocellular; liver neoplasms; lymphoma; magnetic resonance imaging.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


Similar articles
-
Uncommon liver tumors: Case report and literature review.Medicine (Baltimore). 2016 Sep;95(39):e4952. doi: 10.1097/MD.0000000000004952. Medicine (Baltimore). 2016. PMID: 27684838 Free PMC article. Review.
-
MRI features of primary rare malignancies of the liver: A report from four university centres.Eur Radiol. 2018 Apr;28(4):1529-1539. doi: 10.1007/s00330-017-5102-7. Epub 2017 Oct 27. Eur Radiol. 2018. PMID: 29079914
-
Unusual Primary Neoplasms of the Adult Liver: Review of Imaging Appearances and Differential Diagnosis.Curr Probl Diagn Radiol. 2022 Jan-Feb;51(1):73-85. doi: 10.1067/j.cpradiol.2020.10.001. Epub 2020 Nov 2. Curr Probl Diagn Radiol. 2022. PMID: 33199074 Review.
-
Hepatic neoplasms: computed tomography and magnetic resonance features.J Clin Gastroenterol. 2002 Apr;34(4):463-71. doi: 10.1097/00004836-200204000-00019. J Clin Gastroenterol. 2002. PMID: 11907365
-
Hepatocellular carcinoma and other hepatic malignancies: MR imaging.Radiol Clin North Am. 2014 Jul;52(4):683-707. doi: 10.1016/j.rcl.2014.02.015. Epub 2014 Apr 13. Radiol Clin North Am. 2014. PMID: 24889167 Review.
Cited by
-
Advanced diffuse hepatic angiosarcoma treated successfully with TACE and targeted immunotherapy: A case report.Front Oncol. 2023 Apr 20;13:1071403. doi: 10.3389/fonc.2023.1071403. eCollection 2023. Front Oncol. 2023. PMID: 37152029 Free PMC article.
-
Mint3 as a Molecular Target Activated in the Early Stage of Hepatocarcinogenesis.Int J Mol Sci. 2025 Feb 8;26(4):1430. doi: 10.3390/ijms26041430. Int J Mol Sci. 2025. PMID: 40003897 Free PMC article.
-
Diagnostic and prognostic value of microRNAs in cholangiocarcinoma: a systematic review and meta-analysis.Cancer Manag Res. 2018 Jul 18;10:2125-2139. doi: 10.2147/CMAR.S158155. eCollection 2018. Cancer Manag Res. 2018. PMID: 30050323 Free PMC article.
-
Imaging mimickers of cholangiocarcinoma: a pictorial review.Abdom Radiol (NY). 2022 Mar;47(3):981-997. doi: 10.1007/s00261-021-03399-9. Epub 2022 Jan 3. Abdom Radiol (NY). 2022. PMID: 34978593 Review.
References
-
- Global cancer statistics, 2012. Torre LA, Bray F, Siegel RL, et al. CA Cancer J Clin. 2015;65:87–108. - PubMed
-
- Hepatocellular carcinoma: illustrated guide to systematic radiologic diagnosis and staging according to guidelines of the American Association for the study of liver diseases. McEvoy SH, McCarthy CJ, Lavelle LP, et al. RSNA. 2013;33:1653–1668. - PubMed
-
- ACR Manual on Contrast Media Version 10.2. [Jun;2017 ];ACR ACR. https://www.acr.org/Quality-Safety/Resources/Contrast-Manual Media. 2017
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources