

Use of Intraoperative Ultrasound During Spinal Surgery
- PMID: 28989844
- PMCID: PMC5624373
- DOI: 10.1177/2192568217700100
Use of Intraoperative Ultrasound During Spinal Surgery
Abstract
Study design: Review and technical report.
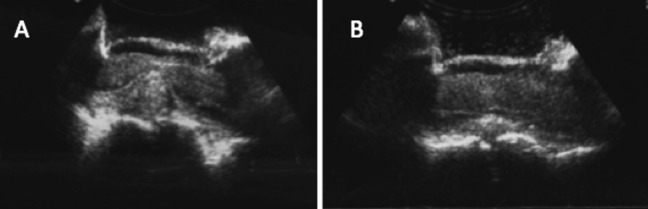
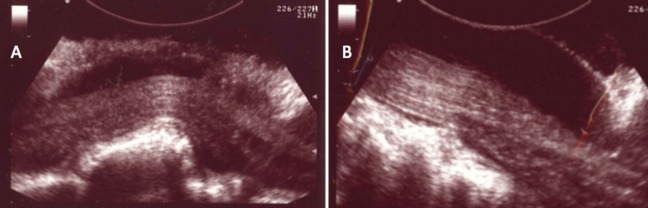
Objective: Intraoperative ultrasound has been used by spine surgeons since the early 1980s. Since that time, more advanced modes of intraoperative imaging and navigation have become widely available. Although the use of ultrasound during spine surgery has fallen out of favor, it remains the only true real-time imaging modality that allows surgeons to visualize soft tissue anatomy instantly and continuously while operating. It is our objective to demonstrate that for this reason, ultrasound is a useful adjunctive technique for spine surgeons, especially when approaching intradural lesions or when addressing pathology in the ventral spinal canal via a posterior approach.
Methods: Using PubMed, the existing literature regarding the use of intraoperative ultrasound during spinal surgery was evaluated. Also, surgical case logs were reviewed to identify spinal operations during which intraoperative ultrasound was used. Illustrative cases were selected and reviewed in detail.
Results: This article provides a brief review of the history of intraoperative ultrasound in spine surgery and describes certain surgical scenarios during which this technique might be useful. Several illustrative cases are provided from our own experience.
Conclusions: Surgeons should consider the use of intraoperative ultrasound when approaching intradural lesions or when addressing pathology ventral to the thecal sac via a posterior approach.
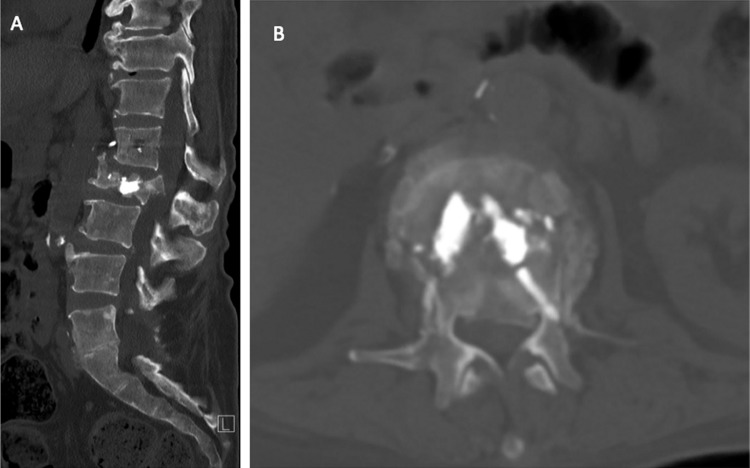
Keywords: intramedullary tumor; intraoperative ultrasound; spine surgery; thoracic disc herniation; thoracolumbar burst fracture.
Conflict of interest statement
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
Similar articles
-
Intraoperative Ultrasound in Spinal Surgery.J Vis Exp. 2022 Aug 17;(186). doi: 10.3791/58080. J Vis Exp. 2022. PMID: 36062998
-
Patient and surgeon radiation exposure during spinal instrumentation using intraoperative computed tomography-based navigation.Spine J. 2016 Mar;16(3):343-54. doi: 10.1016/j.spinee.2015.11.020. Epub 2015 Dec 10. Spine J. 2016. PMID: 26686604
-
Thoracic discectomy by posterior pedicle-sparing, transfacet approach with real-time intraoperative ultrasonography: Clinical article.J Neurosurg Spine. 2014 Oct;21(4):568-76. doi: 10.3171/2014.6.SPINE13682. Epub 2014 Jul 18. J Neurosurg Spine. 2014. PMID: 25036220
-
Intraoperative spinal navigation.Spine (Phila Pa 1976). 2003 Aug 1;28(15 Suppl):S54-61. doi: 10.1097/01.BRS.0000076899.78522.D9. Spine (Phila Pa 1976). 2003. PMID: 12897475 Review.
-
Intraradicular and intradural lumbar disc herniation: experiences with nine cases.Surg Neurol. 1995 Dec;44(6):536-43. doi: 10.1016/0090-3019(95)00248-0. Surg Neurol. 1995. PMID: 8669027 Review.
Cited by
-
Separation surgery for metastatic epidural spinal cord compression: A qualitative review.J Bone Oncol. 2020 Sep 26;25:100320. doi: 10.1016/j.jbo.2020.100320. eCollection 2020 Dec. J Bone Oncol. 2020. PMID: 33088700 Free PMC article. Review.
-
How to Apply Intraoperative Ultrasound when Spinal Trauma Surgery Is Performed in the Lateral Decubitus Position?Orthop Surg. 2024 Feb;16(2):497-505. doi: 10.1111/os.13953. Epub 2023 Dec 4. Orthop Surg. 2024. PMID: 38049386 Free PMC article.
-
Tips and tricks of spinal cord biopsy: insights from a multicenter series of 61 patients.J Neurooncol. 2025 Jul;173(3):719-729. doi: 10.1007/s11060-025-05009-w. Epub 2025 May 14. J Neurooncol. 2025. PMID: 40366520
-
Preliminarily exploring the intraoperative ultrasonography characteristics of patients with degenerative cervical myelopathy.BMC Musculoskelet Disord. 2024 Jul 12;25(1):538. doi: 10.1186/s12891-024-07601-z. BMC Musculoskelet Disord. 2024. PMID: 38997705 Free PMC article.
-
A case of intradural lumbar disc herniation.Clin Case Rep. 2023 Jun 13;11(6):e7514. doi: 10.1002/ccr3.7514. eCollection 2023 Jun. Clin Case Rep. 2023. PMID: 37323261 Free PMC article.
References
-
- Montalvo BM, Quencer RM. Intraoperative sonography in spinal surgery: current state of the art. Neuroradiology. 1986;28:551–590. - PubMed
-
- Rubin JM, Dohrmann GJ. Use of ultrasonically guided probes and catheters in neurosurgery. Surg Neurol. 1982;18:143–148. - PubMed
-
- Raymond CA. Brain, spine surgeons say yes to ultrasound. JAMA. 1986;255:2258–2259. - PubMed
-
- Rubin JM, Dohrmann GJ. The spine and spinal cord during neurosurgical operations: real-time ultrasonography. Radiology. 1985;155:197–200. doi:10.1148/radiology.155.1.3883416. - PubMed
-
- Machi J, Sigel B, Jafar JJ, et al. Criteria for using imaging ultrasound during brain and spinal cord surgery. J Ultrasound Med. 1984;3:155–161. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
