

Comparison Between S2-Alar-Iliac Screw Fixation and Iliac Screw Fixation in Adult Deformity Surgery: Reoperation Rates and Spinopelvic Parameters
- PMID: 28989847
- PMCID: PMC5624376
- DOI: 10.1177/2192568217700111
Comparison Between S2-Alar-Iliac Screw Fixation and Iliac Screw Fixation in Adult Deformity Surgery: Reoperation Rates and Spinopelvic Parameters
Abstract
Study design: Retrospective cohort study.
Objective: The S2-alar-iliac (S2AI) technique has been described as an alternative method for pelvic fixation in place of iliac screws (ISs) in spinal deformity surgery. The objective of this study was to analyze the impact of S2AI screws on radiographical outcomes, including spinopelvic parameters.
Methods: A retrospective review of 17 patients receiving ISs and 46 patients receiving S2AI screws for correction of adult spinal deformity between 2010 and 2015 with minimum 1-year follow-up was conducted. Patient data on postoperative complications, including reoperation rates and proximal junctional kyphosis (PJK), and radiographical parameters was collected and statistically analyzed.
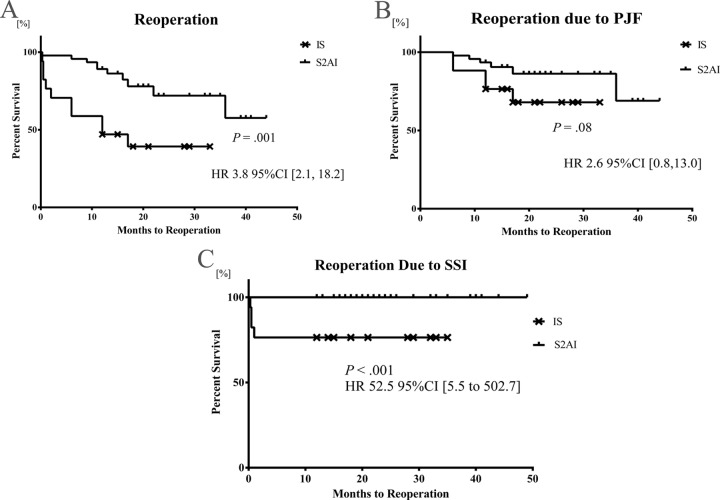
Results: With mean follow-up of 21.1 months, the overall reoperation rate was significantly lower in the S2AI group than in the IS group (21.7% vs 58.8%, P = .01), but the incidence of PJK was similar (32.6% vs 35.3%, P > .99). Moreover, the time to reoperation in the IS group was significantly shorter than in the S2AI group (P = .001), and the S2AI group trended toward a longer time to reoperation due to PJK (P = .08). There was a significantly higher change in pelvic incidence (PI) in the S2AI group (-6.0°) compared with the IS group (P = .001).
Conclusions: Compared with the IS technique, the S2AI technique demonstrated a lower rate of overall reoperation, a similar rate of PJK, longer time to reoperation, and possible reduction in PI. Future studies may be warranted to clarify the mechanism of these results and how they can be translated into improved patient care.
Keywords: S2-alar-iliac screw; iliac screw; lumbar lordosis; lumbosacropelvic fixation; pelvic incidence; proximal junctional failure; proximal junctional kyphosis.
Conflict of interest statement
Declaration of Conflicting Interests: The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Author CRG is a UNCF-Merck Postdoctoral Fellow and is supported by an award from the Burroughs Wellcome Fund. Author AB received a research grant from DePuy Synthes Spine and serves on the clinical advisory board of MedImmune, LLC. Author ZLG has stock ownership in US Spine and Spinal Kinetics, consulting, speaking, and teaching agreements for the AO Foundation, and research support from DePuy Synthes, NREF, AOSpine and AO North America. Author DMS received honoraria from Depuy Synthes, and has had consulting agreements with Medtronic, Globus, Stryker, and Orthofix. Author TFW receives research support from the Gordon and Marilyn Macklin Foundation, and has received complementary research medications from Eli Lilly and Company.
Figures
References
-
- Glattes RC, Bridwell KH, Lenke LG, Kim YJ, Rinella A, Edwards C. Proximal junctional kyphosis in adult spinal deformity following long instrumented posterior spinal fusion: incidence, outcomes, and risk factor analysis. Spine (Phila Pa 1976). 2005;30:1643–1649. - PubMed
-
- Edwards CC, Bridwell KH, Patel A, Rinella AS, Berra A, Lenke LG. Long adult deformity fusions to L5 and the sacrum. A matched cohort analysis. Spine (Phila Pa 1976). 2004;29:1996–2005. - PubMed
-
- Finger T, Bayerl S, Onken J, Czabanka M, Woitzik J, Vajkoczy P. Sacropelvic fixation versus fusion to the sacrum for spondylodesis in multilevel degenerative spine disease. Eur Spine J. 2014;23:1013–1020. doi:10.1007/s00586-014-3165-6. - PubMed
-
- Lowe TG, Kasten MD. An analysis of sagittal curves and balance after Cotrel-Dubousset instrumentation for kyphosis secondary to Scheuermann’s disease. A review of 32 patients. Spine (Phila Pa 1976). 1994;19:1680–1685. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
