

Kinin B1 receptor as a novel, prognostic progression biomarker for carotid atherosclerotic plaques
- PMID: 28990089
- PMCID: PMC5779976
- DOI: 10.3892/mmr.2017.7694
Kinin B1 receptor as a novel, prognostic progression biomarker for carotid atherosclerotic plaques
Abstract
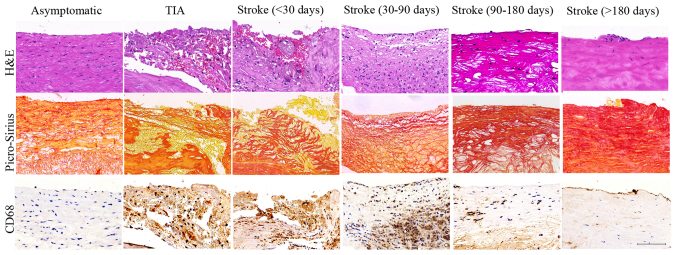
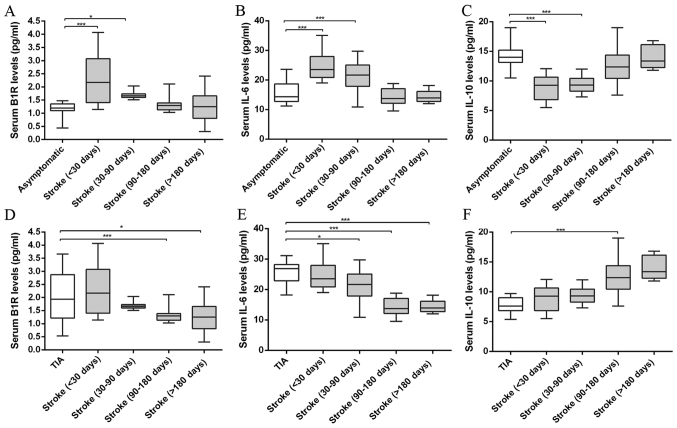
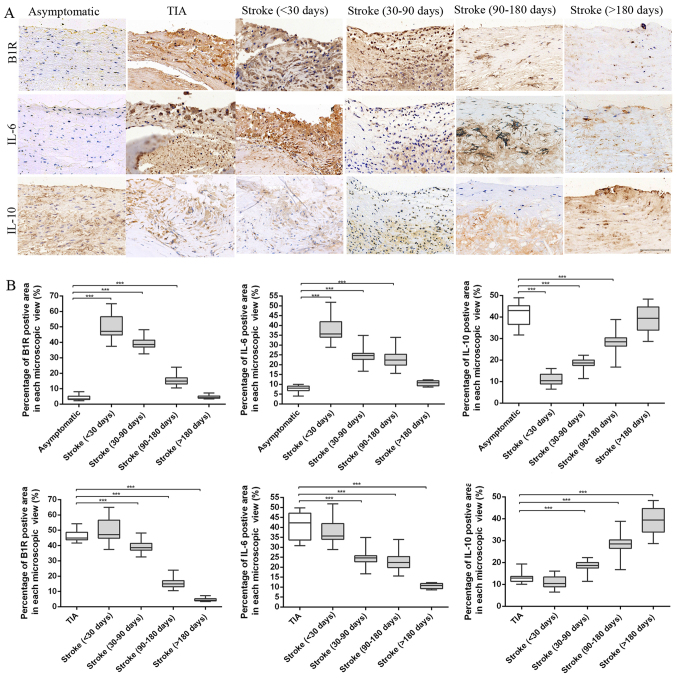
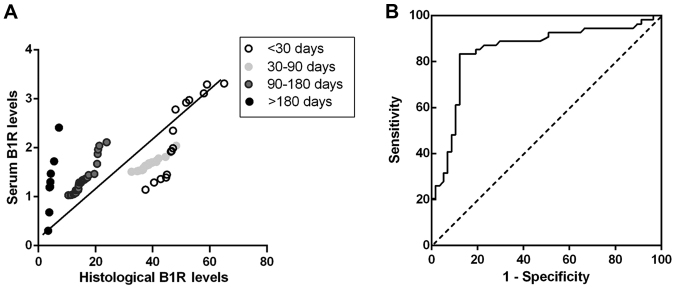
Stroke caused by atherosclerosis remains a leading cause of morbidity and mortality worldwide, associated with carotid plaque rupture and inflammation progression. However, the inflammatory biomarkers which aid in predicting the future course of plaques are less detailed. The present study investigated the association between plaque vulnerable and inflammatory biomarkers using blood and plaque specimens. Carotid plaque specimens were obtained from 80 patients following stroke, 14 patients suffering from transient ischaemic attack and 17 asymptomatic patients that underwent carotid endarterectomy. To assess changes in plaque characteristics at histological levels, plaques were categorized by the time between the latest ischemic stroke and surgical intervention within 30, 30‑90, 90‑180 and over 180 days following stroke. Serum levels of inflammatory biomarkers interleukin (IL)‑6, IL‑10 and kinin B1 receptor (B1R) were measured by ELISA. Histological assessment of plaque was used to evaluate the plaque stability, progression and the inflammatory biomarker levels. Comparisons of histological characteristics demonstrated that plaques revealed an unstable phenotype following stroke within 30, 30‑90 days and then remodeled into more stable plaques following stroke at 90‑180 and over 180 days. By comparing the serum levels of inflammatory biomarkers, it was observed that IL‑6 and B1R levels tended to decline whereas IL‑10 levels increased in stroke patients from <30 days to over 180 days. Immunohistochemical analysis of IL‑6, IL‑10 and B1R demonstrated similar alterations in serum levels. Correlation analyses revealed that only B1R serum level was significantly correlated with histological level in patients with carotid atherosclerosis. The findings revealed that serum B1R levels may provide prognostic information and currently act as potential indicators for progression in atherosclerosis.
Figures
References
-
- Tuttolomondo A, Pecoraro R, Casuccio A, Di Raimondo D, Buttà C, Clemente G, Corte V Della, Guggino G, Arnao V, Maida C, et al. Peripheral frequency of CD4+ CD28- cells in acute ischemic stroke: Relationship with stroke subtype and severity markers. Medicine (Baltimore) 2015;94:e813. doi: 10.1097/MD.0000000000000813. - DOI - PMC - PubMed
-
- Tuttolomondo A, Pedone C, Pinto A, Di Raimondo D, Fernandez P, Di Sciacca R, Licata G. Gruppo Italiano di Farmacoepidemiologia dell'Anziano (GIFA) researchers: Predictors of outcome in acute ischemic cerebrovascular syndromes: The GIFA study. Int J Cardiol. 2008;125:391–396. doi: 10.1016/j.ijcard.2007.03.109. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
