

Effect of Chronic Kidney Disease on Nonrenal Elimination Pathways: A Systematic Assessment of CYP1A2, CYP2C8, CYP2C9, CYP2C19, and OATP
- PMID: 28990182
- PMCID: PMC5947523
- DOI: 10.1002/cpt.807
Effect of Chronic Kidney Disease on Nonrenal Elimination Pathways: A Systematic Assessment of CYP1A2, CYP2C8, CYP2C9, CYP2C19, and OATP
Abstract
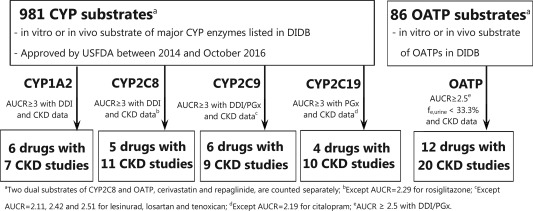
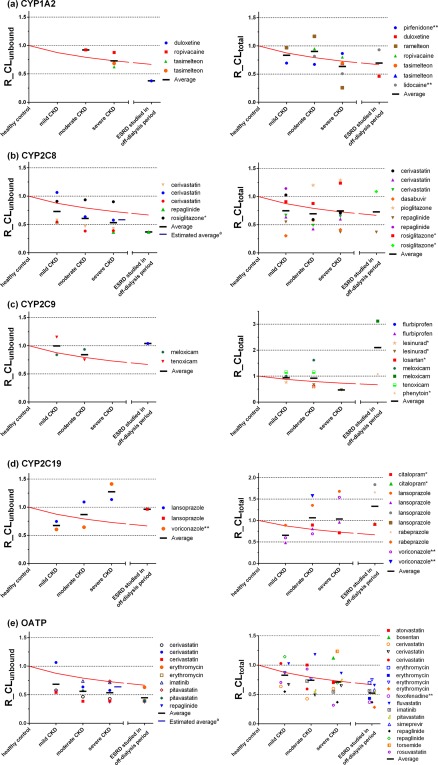
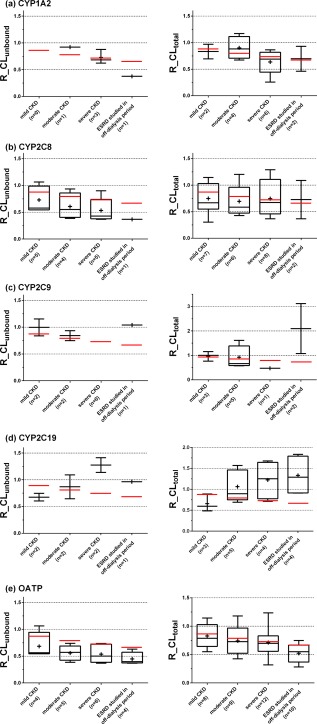
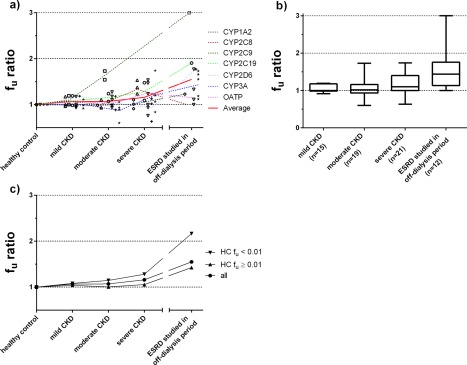
Our recent studies have shown that chronic kidney disease (CKD) affects the pharmacokinetics (PKs) of cytochrome P450 (CYP)2D6-metabolized drugs, whereas effects were less evident on CYP3A4/5. Therefore, the effect of CKD on the disposition of CYP1A2-metabolized, CYP2C8-metabolized, CYP2C9-metabolized, CYP2C19-metabolized, and organic anion-transporting polypeptide (OATP)-transported drugs was investigated. We identified dedicated CKD studies with 6, 5, 6, 4, and 12 "model" substrates for CYP1A2, CYP2C8, CYP2C9, CYP2C19, and OATP, respectively. Our analyses suggest that clearance of OATP substrates decreases as kidney function declines. Similar trends were seen for CYP2C8; but overlap between some CYP2C8 and OATP substrates highlights that their interplay needs further investigation. In contrast, the effect of CKD on CYP1A2, CYP2C9, and CYP2C19 was variable and modest compared to CYP2C8 and OATP. This improved understanding of elimination-pathway-dependency in CKD is important to inform the need and conduct of PK studies in these patients for nonrenally eliminated drugs.
Published 2017. This article is a U.S. Government work and is in the public domain in the USA. Clinical Pharmacology & Therapeutics published by Wiley Periodicals, Inc. on behalf of American Society for Clinical Pharmacology and Therapeutics.
Figures
References
-
- Ladda, M.A. & Goralski, K.B. The effects of CKD on cytochrome P450‐mediated drug metabolism. Adv. Chronic Kidney Dis. 23, 67–75 (2016). - PubMed
-
- Jha, V. et al Chronic kidney disease: global dimension and perspectives. Lancet 382, 260–272 (2013). - PubMed
-
- Chen, Y.C. et al Risk factors associated with adverse drug events among older adults in emergency department. Eur. J. Intern. Med. 25, 49–55 (2014). - PubMed
-
- Nolin, T.D. , Naud, J. , Leblond, F.A. & Pichette, V. Emerging evidence of the impact of kidney disease on drug metabolism and transport. Clin. Pharmacol. Ther. 83, 898–903 (2008). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
