

Physiological dead space and arterial carbon dioxide contributions to exercise ventilatory inefficiency in patients with reduced or preserved ejection fraction heart failure
- PMID: 28990307
- PMCID: PMC5741513
- DOI: 10.1002/ejhf.913
Physiological dead space and arterial carbon dioxide contributions to exercise ventilatory inefficiency in patients with reduced or preserved ejection fraction heart failure
Abstract
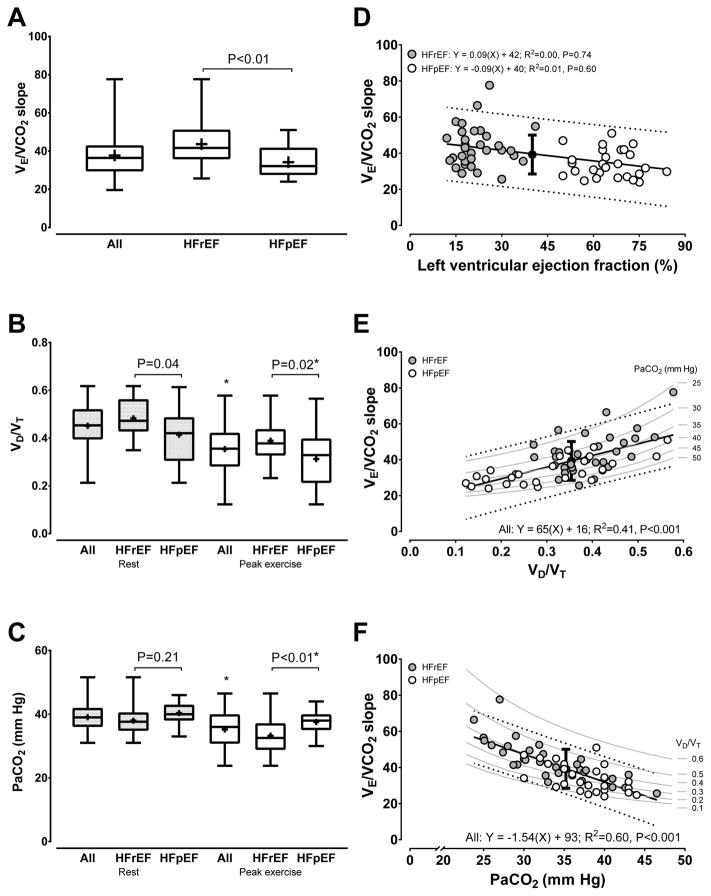
Aims: Patients with heart failure (HF) with reduced (HFrEF) or preserved (HFpEF) ejection fraction demonstrate an increased ventilatory equivalent for carbon dioxide (V̇E /V̇CO2 ) slope. The physiological correlates of the V̇E /V̇CO2 slope remain unclear in the two HF phenotypes. We hypothesized that changes in the physiological dead space to tidal volume ratio (VD /VT ) and arterial CO2 tension (PaCO2 ) differentially contribute to the V̇E /V̇CO2 slope in HFrEF vs. HFpEF.
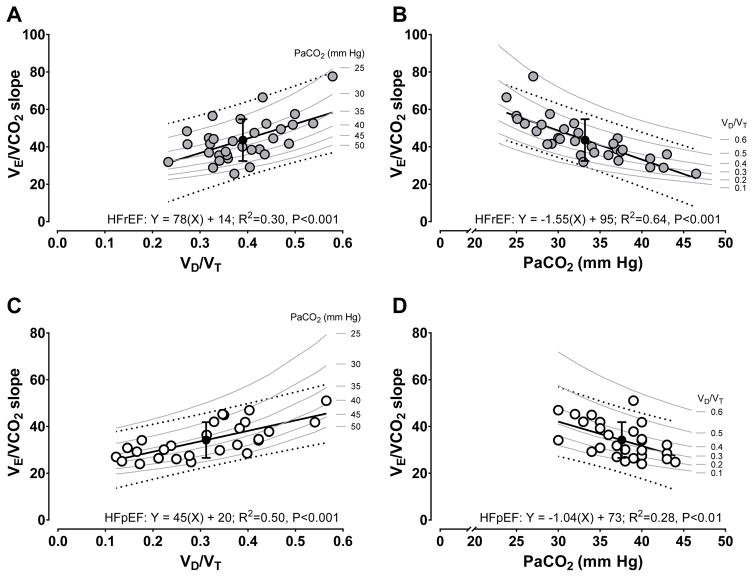
Methods and results: Adults with HFrEF (n = 32) and HFpEF (n = 27) [mean ± standard deviation (SD) left ventricular ejection fraction: 22 ± 7% and 61 ± 9%, respectively; mean ± SD body mass index: 28 ± 4 kg/m2 and 33 ± 6 kg/m2 , respectively; P < 0.01] performed cardiopulmonary exercise testing with breath-by-breath ventilation and gas exchange measurements. PaCO2 was measured via radial arterial catheterization. We calculated the V̇E /V̇CO2 slope via linear regression, and VD /VT = 1 - [(863 × V̇CO2 )/(V̇E × PaCO2 )]. Resting VD /VT (0.48 ± 0.08 vs. 0.41 ± 0.11; P = 0.04), but not PaCO2 (38 ± 5 mmHg vs. 40 ± 3 mmHg; P = 0.21) differed between HFrEF and HFpEF. Peak exercise VD /VT (0.39 ± 0.08 vs. 0.32 ± 0.12; P = 0.02) and PaCO2 (33 ± 6 mmHg vs. 38 ± 4 mmHg; P < 0.01) differed between HFrEF and HFpEF. The V̇E /V̇CO2 slope was higher in HFrEF compared with HFpEF (44 ± 11 vs. 35 ± 8; P < 0.01). Variance associated with the V̇E /V̇CO2 slope in HFrEF and HFpEF was explained by peak exercise VD /VT (R2 = 0.30 and R2 = 0.50, respectively) and PaCO2 (R2 = 0.64 and R2 = 0.28, respectively), but the relative contributions of each differed (all P < 0.01).
Conclusions: Relationships between the V̇E /V̇CO2 slope and both VD /VT and PaCO2 are robust, but differ between HFpEF and HFrEF. Increasing V̇E /V̇CO2 slope appears to be strongly explained by mechanisms influential in regulating PaCO2 in HFrEF, which contrasts with the strong role of increased VD /VT in HFpEF.
Keywords: Cardiopulmonary exercise testing; Exercise capacity; Exercise intolerance; Exercise tolerance; Exercise ventilatory efficiency; Heart failure with preserved ejection fraction.
© 2017 The Authors. European Journal of Heart Failure © 2017 European Society of Cardiology.
Conflict of interest statement
Figures
Comment in
-
Exercise ventilatory inefficiency in heart failure: some fresh news into the roadmap of heart failure with preserved ejection fraction phenotyping.Eur J Heart Fail. 2017 Dec;19(12):1686-1689. doi: 10.1002/ejhf.940. Epub 2017 Oct 9. Eur J Heart Fail. 2017. PMID: 28990273 No abstract available.
References
-
- Guazzi M, Myers J, Arena R. Cardiopulmonary exercise testing in the clinical and prognostic assessment of diastolic heart failure. J Am Coll Cardiol. 2005 Nov 15;46(10):1883–1890. - PubMed
-
- Shafiq A, Brawner CA, Aldred HA, Lewis B, Williams CT, Tita C, Schairer JR, Ehrman JK, Velez M, Selektor Y, Lanfear DE, Keteyian SJ. Prognostic value of cardiopulmonary exercise testing in heart failure with preserved ejection fraction. The Henry Ford HospITal CardioPulmonary EXercise Testing (FIT-CPX) project. Am Heart J. 2016 Apr;174:167–172. - PMC - PubMed
-
- Nedeljkovic I, Banovic M, Stepanovic J, Giga V, Djordjevic-Dikic A, Trifunovic D, Nedeljkovic M, Petrovic M, Dobric M, Dikic N, Zlatar M, Beleslin B. The combined exercise stress echocardiography and cardiopulmonary exercise test for identification of masked heart failure with preserved ejection fraction in patients with hypertension. Eur J Prev Cardiol. 2016 Jan;23(1):71–77. - PubMed
-
- Guazzi M, Reina G, Tumminello G, Guazzi MD. Exercise ventilation inefficiency and cardiovascular mortality in heart failure: the critical independent prognostic value of the arterial CO2 partial pressure. Eur Heart J. 2005 Mar;26(5):472–480. [Research Support, Non-U.S. Gov’t] - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
