

Malaria Control Interventions Contributed to Declines in Malaria Parasitemia, Severe Anemia, and All-Cause Mortality in Children Less Than 5 Years of Age in Malawi, 2000-2010
- PMID: 28990920
- PMCID: PMC5619935
- DOI: 10.4269/ajtmh.17-0203
Malaria Control Interventions Contributed to Declines in Malaria Parasitemia, Severe Anemia, and All-Cause Mortality in Children Less Than 5 Years of Age in Malawi, 2000-2010
Abstract
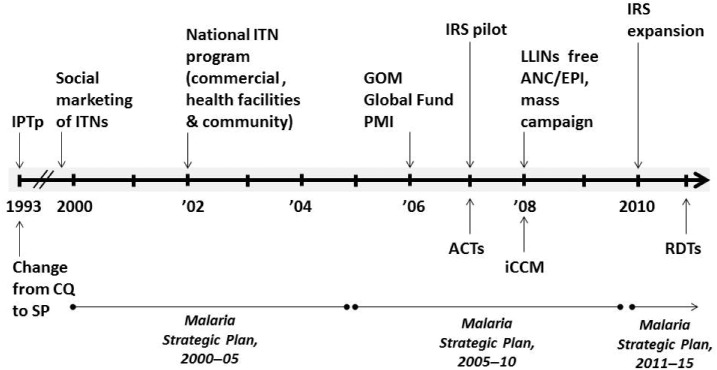
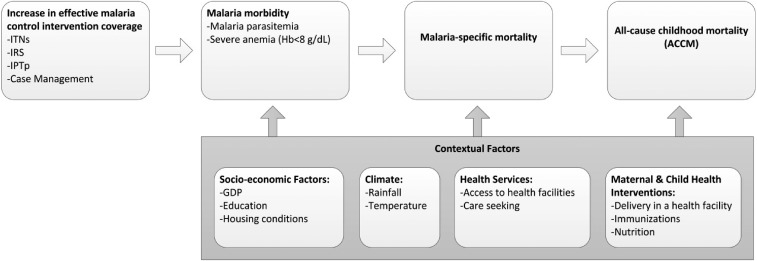
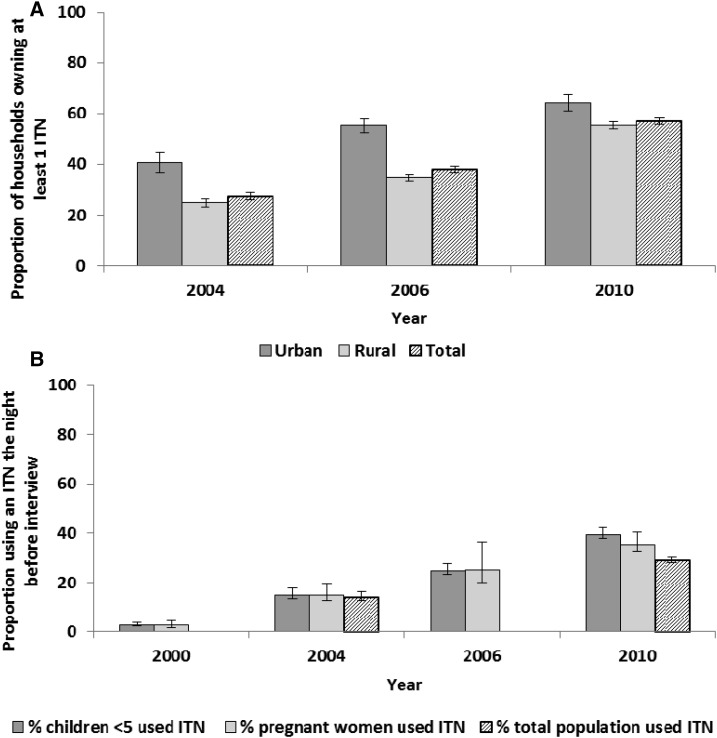
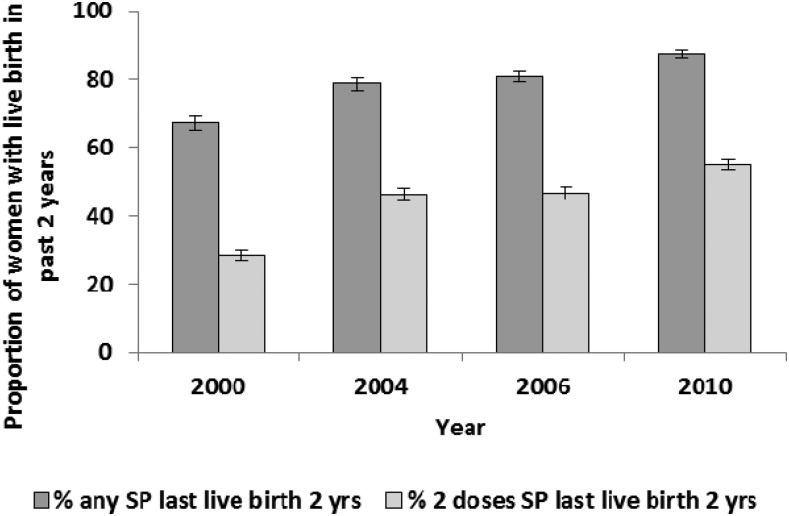
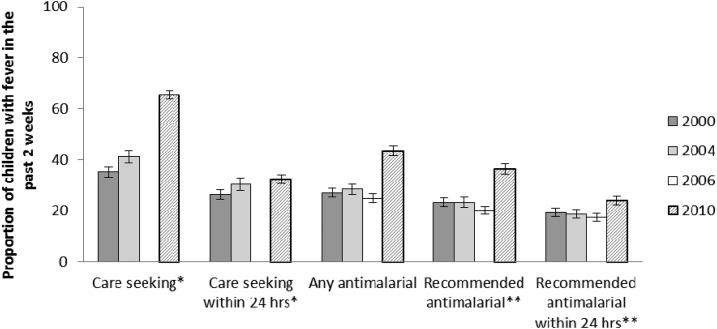
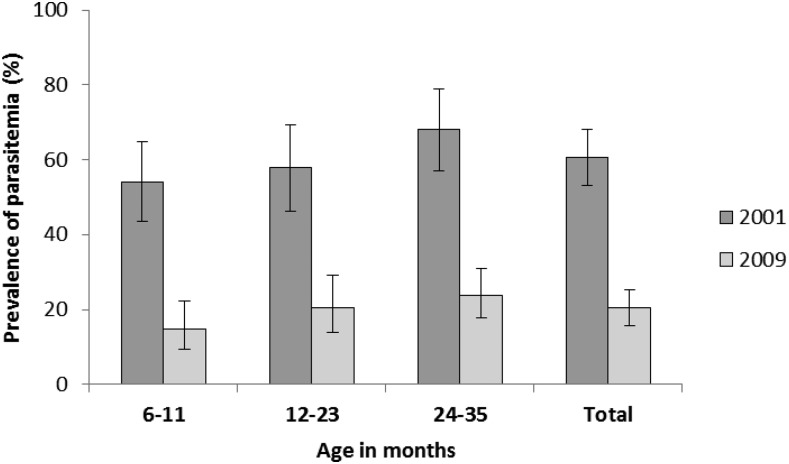
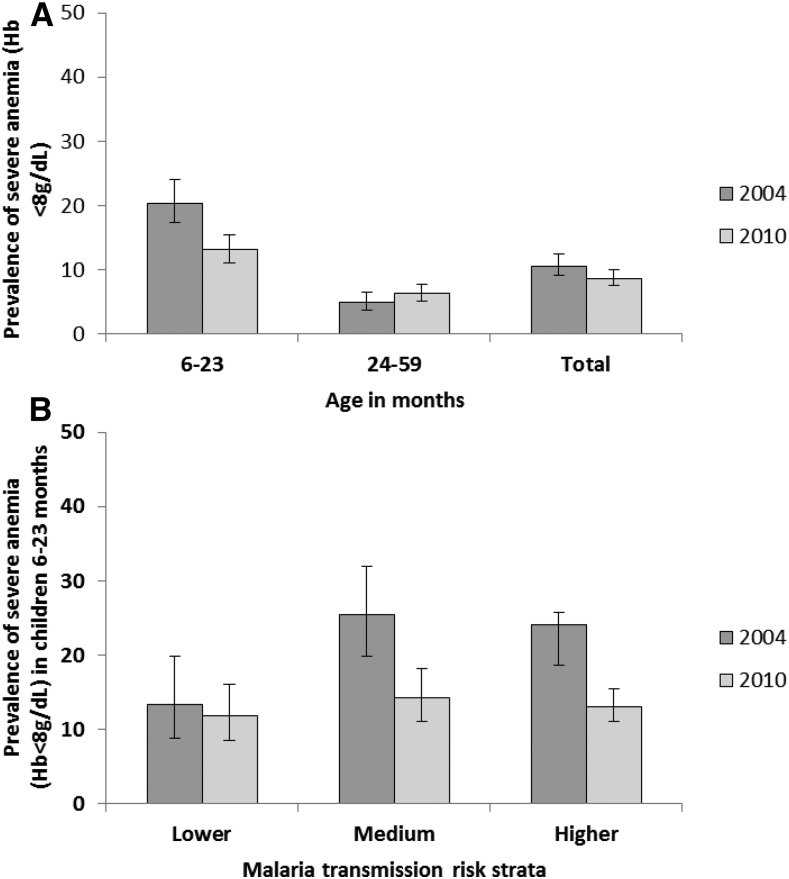
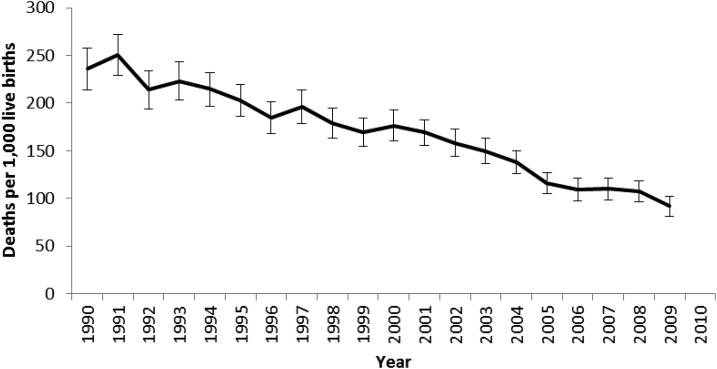
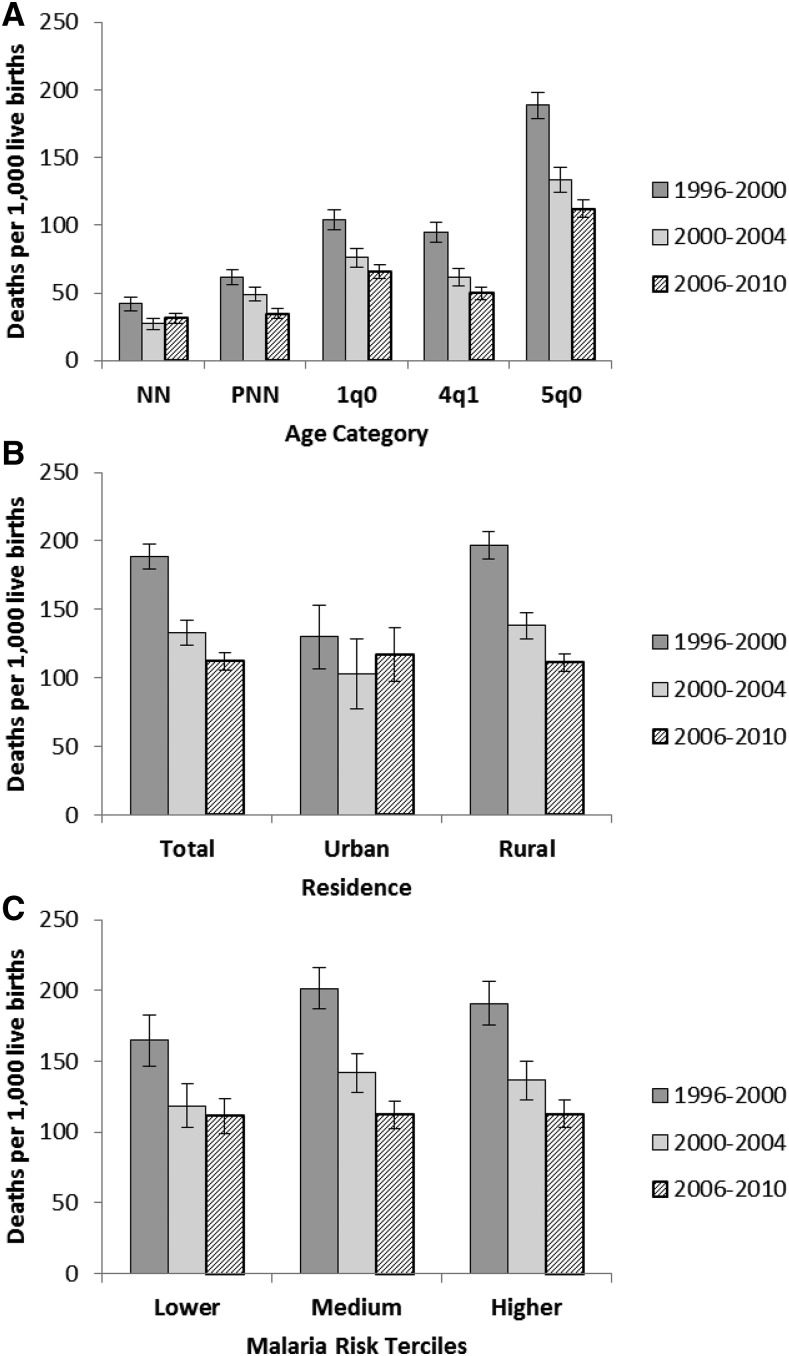
Malaria control intervention coverage increased nationwide in Malawi during 2000-2010. Trends in intervention coverage were assessed against trends in malaria parasite prevalence, severe anemia (hemoglobin < 8 g/dL), and all-cause mortality in children under 5 years of age (ACCM) using nationally representative household surveys. Associations between insecticide-treated net (ITN) ownership, malaria morbidity, and ACCM were also assessed. Household ITN ownership increased from 27.4% (95% confidence interval [CI] = 25.9-29.0) in 2004 to 56.8% (95% CI = 55.6-58.1) in 2010. Similarly intermittent preventive treatment during pregnancy coverage increased from 28.2% (95% CI = 26.7-29.8) in 2000 to 55.0% (95% CI = 53.4-56.6) in 2010. Malaria parasite prevalence decreased significantly from 60.5% (95% CI = 53.0-68.0) in 2001 to 20.4% (95% CI = 15.7-25.1) in 2009 in children aged 6-35 months. Severe anemia prevalence decreased from 20.4% (95% CI: 17.3-24.0) in 2004 to 13.1% (95% CI = 11.0-15.4) in 2010 in children aged 6-23 months. ACCM decreased 41%, from 188.6 deaths per 1,000 live births (95% CI = 179.1-198.0) during 1996-2000, to 112.1 deaths per 1,000 live births (95% CI = 105.8-118.5) during 2006-2010. When controlling for other covariates in random effects logistic regression models, household ITN ownership was protective against malaria parasitemia in children (odds ratio [OR] = 0.81, 95% CI = 0.72-0.92) and severe anemia (OR = 0.82, 95% CI = 0.72-0.94). After considering the magnitude of changes in malaria intervention coverage and nonmalaria factors, and given the contribution of malaria to all-cause mortality in malaria-endemic countries, the substantial increase in malaria control interventions likely improved child survival in Malawi during 2000-2010.
Figures
References
-
- National Malaria Control Programme, 2001. Malaria Strategic Plan 2001–2005: Scaling up Malaria Control Interventions Malawi. Lilongwe, Malawi: Government of Malawi Ministry of Health.
-
- Malawi Malaria Impact Evaluation Group, 2016. Evaluation of the Impact of Malaria Control Interventions on All-Cause Mortality in Children Under-Five in Malawi. Washington, DC: President’s Malaria Intiative.
-
- World Health Organization (WHO), 2011. World Malaria Report 2011. Geneva, Switzerland: World Health Organization.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
