

Associations of Muscle Mass and Strength with All-Cause Mortality among US Older Adults
- PMID: 28991040
- PMCID: PMC5820209
- DOI: 10.1249/MSS.0000000000001448
Associations of Muscle Mass and Strength with All-Cause Mortality among US Older Adults
Abstract
Introduction: Recent studies suggested that muscle mass and muscle strength may independently or synergistically affect aging-related health outcomes in older adults; however, prospective data on mortality in the general population are sparse.
Methods: We aimed to prospectively examine individual and joint associations of low muscle mass and low muscle strength with all-cause mortality in a nationally representative sample. This study included 4449 participants age 50 yr and older from the National Health and Nutrition Examination Survey 1999 to 2002 with public use 2011 linked mortality files. Weighted multivariable logistic regression models were adjusted for age, sex, race, body mass index (BMI), smoking, alcohol use, education, leisure time physical activity, sedentary time, and comorbid diseases.
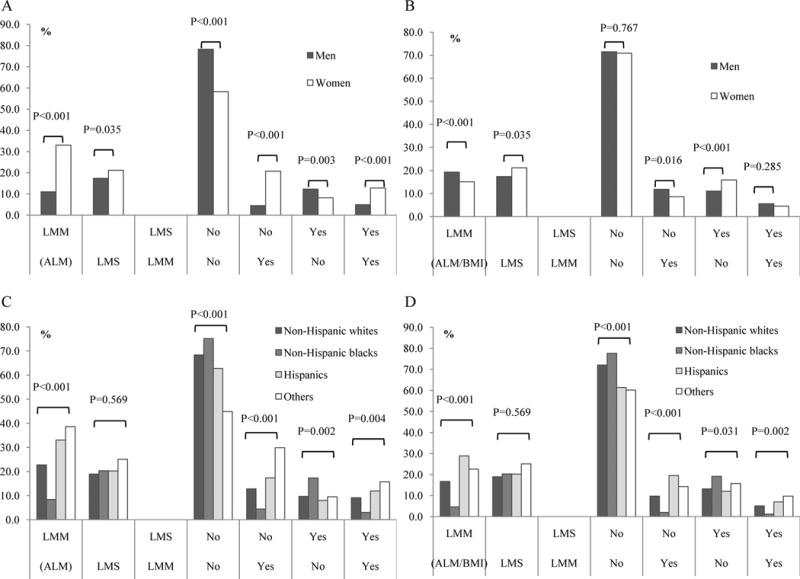
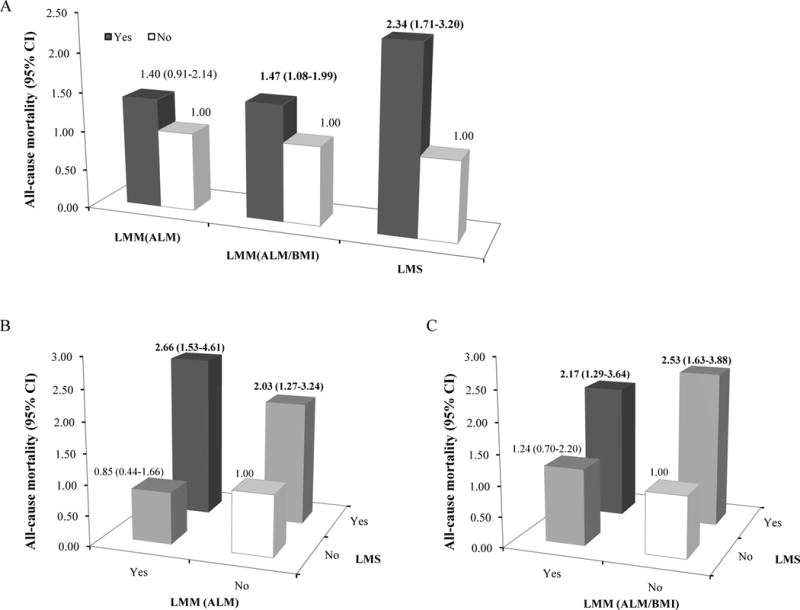
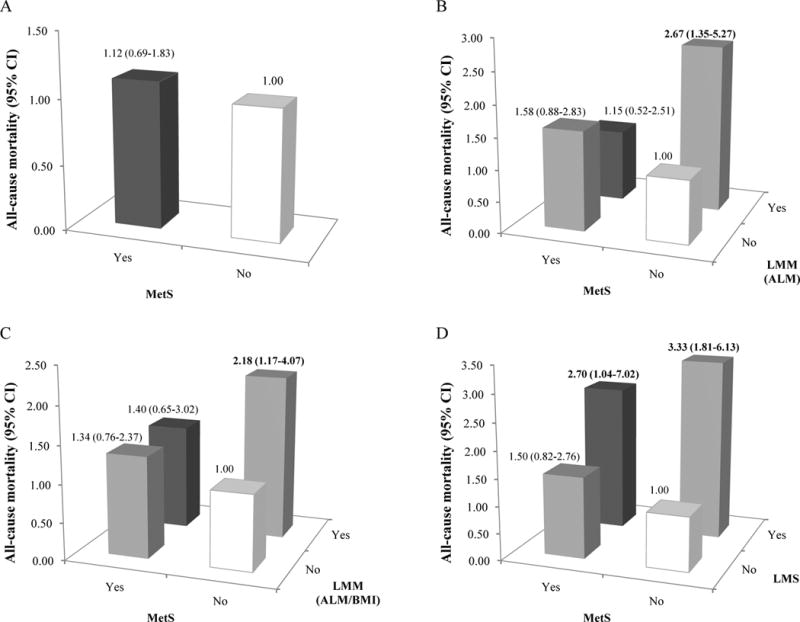
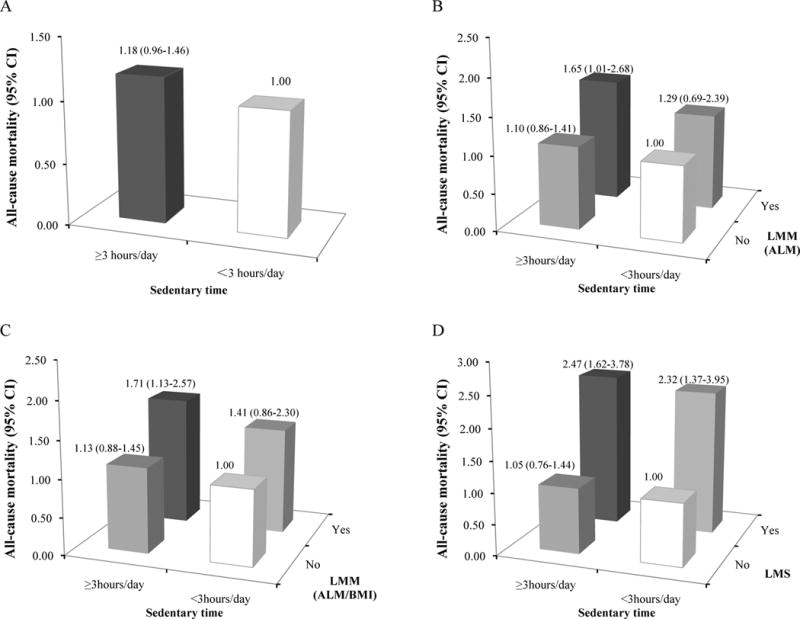
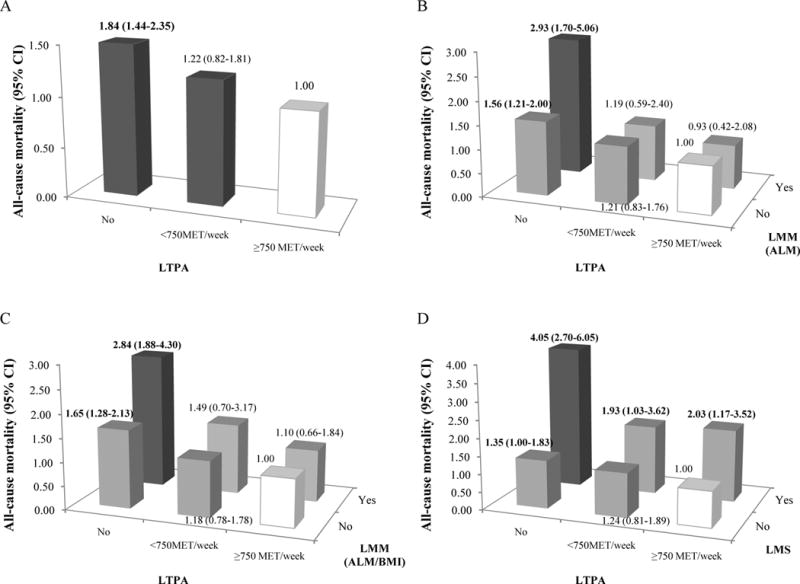
Results: Overall, the prevalence of low muscle mass was 23.1% defined by appendicular lean mass (ALM) and 17.0% defined by ALM/BMI, and the prevalence of low muscle strength was 19.4%. In the joint analyses, all-cause mortality was significantly higher among individuals with low muscle strength, whether they had low muscle mass (odds ratio [OR], 2.03; 95% confidence interval [CI], 1.27-3.24 for ALM; OR, 2.53; 95% CI, 1.64-3.88 for ALM/BMI) or not (OR, 2.66; 95% CI, 1.53-4.62 for ALM; OR, 2.17; 95% CI, 1.29-3.64 for ALM/BMI). In addition, the significant associations between low muscle strength and all-cause mortality persisted across different levels of metabolic syndrome, sedentary time, and LTPA.
Conclusions: Low muscle strength was independently associated with elevated risk of all-cause mortality, regardless of muscle mass, metabolic syndrome, sedentary time, or LTPA among US older adults, indicating the importance of muscle strength in predicting aging-related health outcomes in older adults.
Figures
References
-
- Rosenberg IH. Sarcopenia: origins and clinical relevance. J Nutr. 1997;127(5 Suppl):990S–1S. - PubMed
-
- Goodpaster BH, Park SW, Harris TB, et al. The loss of skeletal muscle strength, mass, and quality in older adults: the health, aging and body composition study. J Gerontol A Biol Sci Med Sci. 2006;61(10):1059–64. - PubMed
-
- Cawthon PM, Marshall LM, Michael Y, et al. Frailty in older men: prevalence, progression, and relationship with mortality. J Am Geriatr Soc. 2007;55(8):1216–23. - PubMed
-
- Batsis JA, Mackenzie TA, Barre LK, Lopez-Jimenez F, Bartels SJ. Sarcopenia, sarcopenic obesity and mortality in older adults: results from the National Health and Nutrition Examination Survey III. Eur J Clin Nutr. 2014;68(9):1001–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
