

Clinical and imaging correlation in patients with pathologically confirmed tumefactive demyelinating lesions
- PMID: 28991721
- PMCID: PMC5659762
- DOI: 10.1016/j.jns.2017.08.015
Clinical and imaging correlation in patients with pathologically confirmed tumefactive demyelinating lesions
Abstract
Objectives: To characterize clinical and imaging features in patients with pathologically confirmed demyelinating lesions.
Methods: In this retrospective chart review, we analyzed clinical-radiological-pathological correlations in patients >15years old who underwent brain biopsy at our institution between 2000 and 2015 and had inflammatory demyelination on neuropathology.
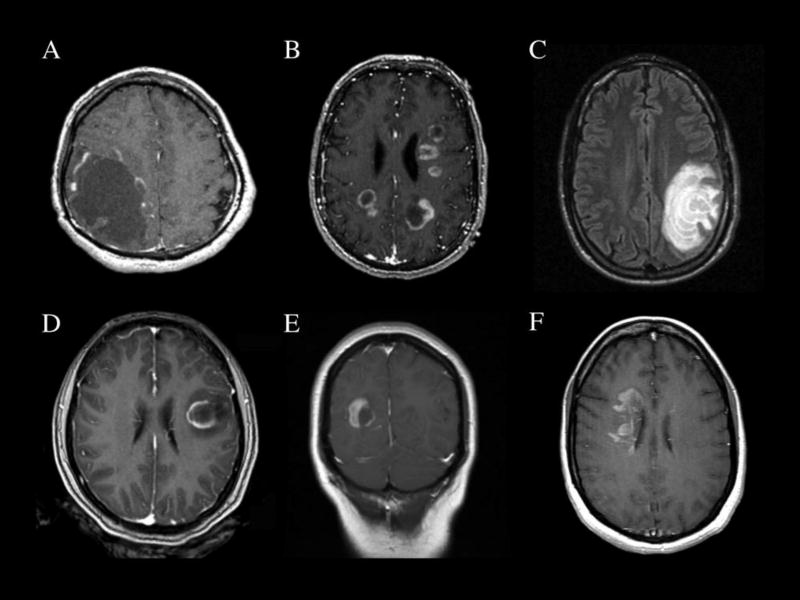
Results: Of 31 patients, the mean age was 42years (range 16 to 69years) and 55% were female. All but one of the biopsied lesions were considered tumefactive demyelinating lesions (TDLs) by imaging criteria, measuring >2cm on contrast-enhanced brain MRI. On clinical follow-up, the final diagnosis was a CNS malignancy in 2 patients (6.5%). In patients without malignant tumor, the TDL was solitary in 12 (41%) and multifocal in 17 (59%), with contrast enhancement in all but one case, primarily in an incomplete rim enhancement pattern (75.9%). Of 16 patients with at least 12months of clinical follow-up, 7 (43.8%) had a clinical relapse. Of patients without a prior neurologic history, relapse occurred in 2/7 (29%) in solitary TDL and 2/6 (33%) in multifocal lesions at initial presentation. Recurrent TDLs occurred in 3 patients, all with initially solitary TDLs. Stratifying by CSF analysis, 4 of 6 patients (67%) with either an elevated IgG Index or >2 oligoclonal bands suffered a clinical relapse compared to 2/8 (25%) with non-inflammatory CSF.
Conclusions: Pathologically confirmed TDLs call for careful clinical correlation, clinical follow-up and imaging surveillance. Although sometimes clinically monophasic, tumefactive demyelinating lesions carried nearly a 45% risk of near-term clinical relapse in our study, even when presenting initially as a solitary mass lesion.
Keywords: Brain biopsy; Demyelination; MRI; Multiple sclerosis; Neuropathology; Tumefactive.
Copyright © 2017 Elsevier B.V. All rights reserved.
Figures
References
-
- Lucchinetti CF, Gavrilova RH, Metz I, Parisi JE, Scheithauer BW, Weigand S, Thomsen K, Mandrekar J, Altintas A, Erickson BJ, König F, Giannini C, Lassmann H, Linbo L, Pittock SJ, Brück W. Clinical and radiographic spectrum of pathologically confirmed tumefactive multiple sclerosis. Brain. 2008;131:1759–1775. doi: 10.1093/brain/awn098. - DOI - PMC - PubMed
-
- Mabray MC, Cohen BA, Villanueva-Meyer JE, Valles FE, Barajas RF, Rubenstein JL, Cha S. Performance of apparent diffusion coefficient values and conventional MRI features in differentiating tumefactive demyelinating lesions from primary brain neoplasms. Am. J. Roentgenol. 2015;205:1075–1085. doi: 10.2214/AJR.14.13970. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
