

Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: A consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imaging (EACVI)
- PMID: 28992817
- PMCID: PMC5633041
- DOI: 10.1186/s12968-017-0389-8
Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: A consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imaging (EACVI)
Erratum in
-
Correction to: Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: A consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imaging (EACVI).J Cardiovasc Magn Reson. 2018 Feb 7;20(1):9. doi: 10.1186/s12968-017-0408-9. J Cardiovasc Magn Reson. 2018. PMID: 29415744 Free PMC article.
Abstract
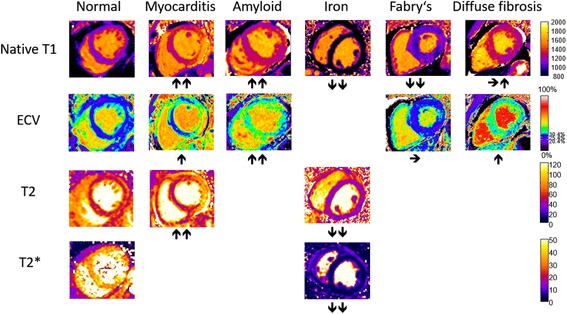
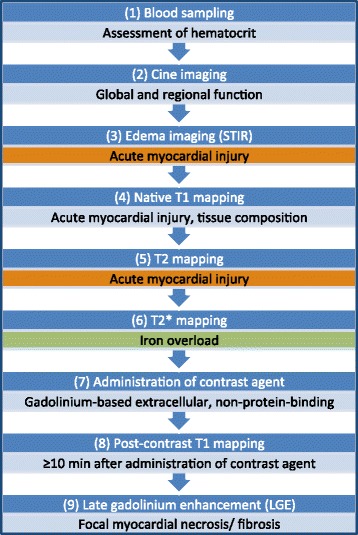
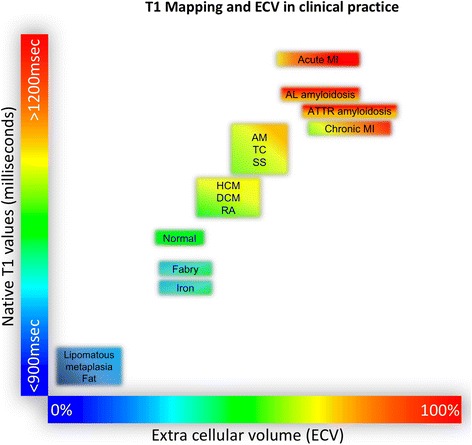
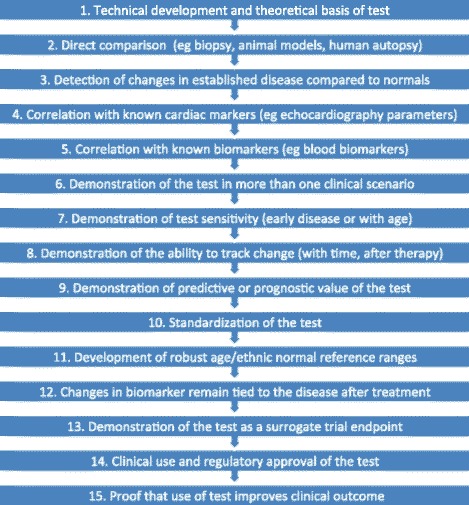
Parametric mapping techniques provide a non-invasive tool for quantifying tissue alterations in myocardial disease in those eligible for cardiovascular magnetic resonance (CMR). Parametric mapping with CMR now permits the routine spatial visualization and quantification of changes in myocardial composition based on changes in T1, T2, and T2*(star) relaxation times and extracellular volume (ECV). These changes include specific disease pathways related to mainly intracellular disturbances of the cardiomyocyte (e.g., iron overload, or glycosphingolipid accumulation in Anderson-Fabry disease); extracellular disturbances in the myocardial interstitium (e.g., myocardial fibrosis or cardiac amyloidosis from accumulation of collagen or amyloid proteins, respectively); or both (myocardial edema with increased intracellular and/or extracellular water). Parametric mapping promises improvements in patient care through advances in quantitative diagnostics, inter- and intra-patient comparability, and relatedly improvements in treatment. There is a multitude of technical approaches and potential applications. This document provides a summary of the existing evidence for the clinical value of parametric mapping in the heart as of mid 2017, and gives recommendations for practical use in different clinical scenarios for scientists, clinicians, and CMR manufacturers.
Conflict of interest statement
Authors’ information
Not applicable.
Consent for publication
All authors have read and approved the final version of this manuscript.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Moon JC, Messroghli DR, Kellman P, Piechnik SK, Robson MD, Ugander M, et al. Myocardial T1 mapping and extracellular volume quantification: a Society for Cardiovascular Magnetic Resonance (SCMR) and CMR Working Group of the European Society of Cardiology consensus statement. J Cardiovasc Magn Reson. 2013;15:92. - PMC - PubMed
-
- Messroghli DR, Radjenovic A, Kozerke S, Higgins DM, Sivananthan MU, Ridgway JP. Modified Look-Locker inversion recovery (MOLLI) for high-resolution T1 mapping of the heart. Magn Reson Med. 2004;52:141–146. - PubMed
-
- Messroghli DR, Plein S, Higgins DM, Walters K, Jones TR, Ridgway JP, et al. Human myocardium: single-breath-hold MR T1 mapping with high spatial resolution--reproducibility study. Radiology. 2006;238:1004–1012. - PubMed
-
- Messroghli DR, Greiser A, Fröhlich M, Dietz R, Schulz-Menger J. Optimization and validation of a fully-integrated pulse sequence for modified look-locker inversion-recovery (MOLLI) T1 mapping of the heart. J Magn Reson Imaging. 2007;26:1081–1086. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
