

Delayed spinal cord infarction following anterior cervical surgical decompression
- PMID: 28993348
- PMCID: PMC5652393
- DOI: 10.1136/bcr-2017-219863
Delayed spinal cord infarction following anterior cervical surgical decompression
Abstract
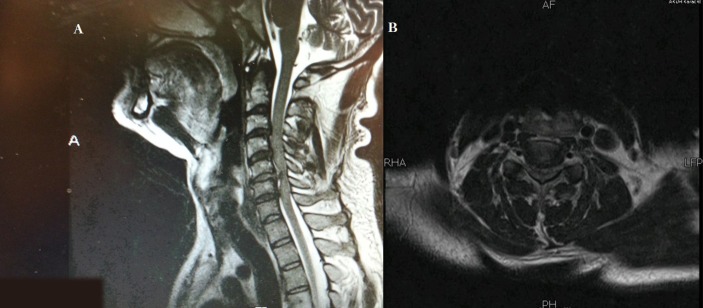
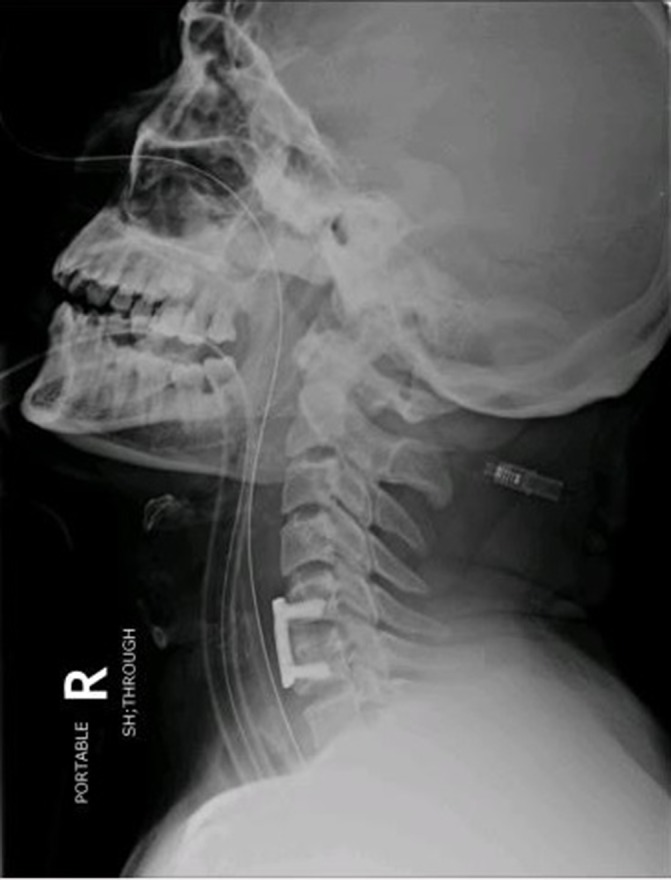
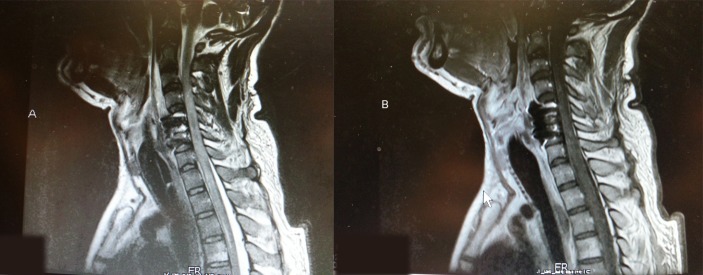
Anterior cervical discectomy and fusion (ACDF) for cord compression is a safe and effective procedure with good outcomes. However, worsening of myelopathy is the most feared adverse event of the surgery. We report the case of a 36-year-old male patient who presented with an acute non-traumatic C5-6 cervical disc herniation causing incomplete quadriparesis. He underwent an uncomplicated ACDF at C5-6, and after an initial period of improvement, he developed a delayed onset of an anterior cord syndrome on day 3, without any discerning cause. We have reviewed similar cases reported in the literature and believe that our patient's postsurgical course is consistent with a delayed ischaemic/reperfusion injury to the cord following surgical decompression and restoration of blood flow through the anterior spinal artery and we make suggestions for management of such clinical events.
Keywords: mechanical ventilation; neuroimaging; neurological injury; neurosurgery; spinal cord.
© BMJ Publishing Group Ltd (unless otherwise stated in the text of the article) 2017. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Goh HK, Li YH. Non-traumatic acute paraplegia caused by cervical disc herniation in a patient with sleep apnoea. Singapore Med J 2004;45:235–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous