

Hoarseness as a presentation of mycosis fungoides infiltrating the larynx
- PMID: 28993359
- PMCID: PMC5652520
- DOI: 10.1136/bcr-2017-221531
Hoarseness as a presentation of mycosis fungoides infiltrating the larynx
Abstract
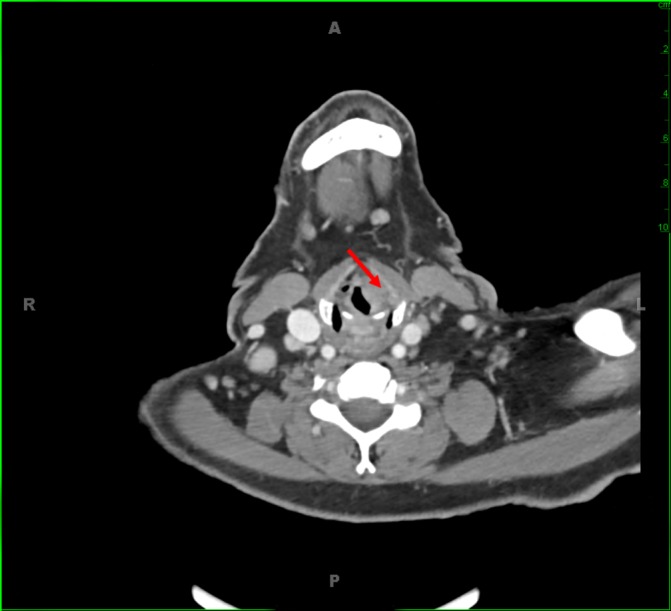
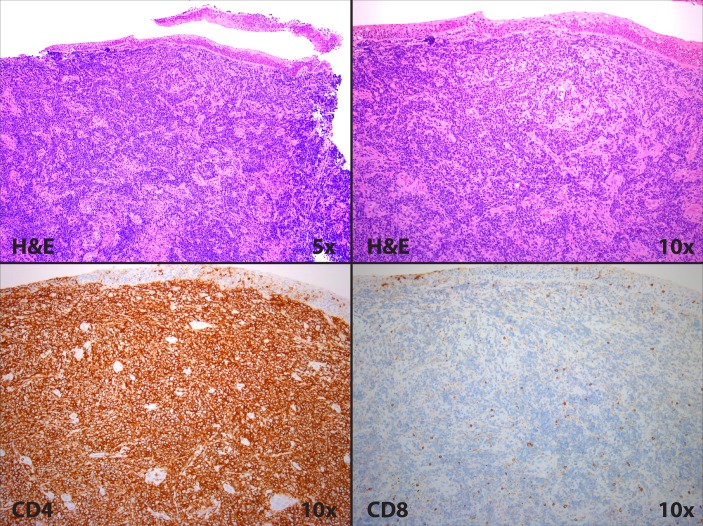
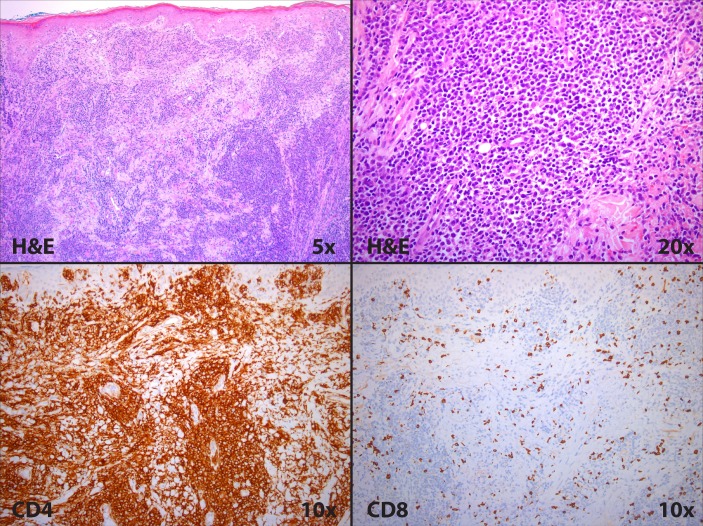
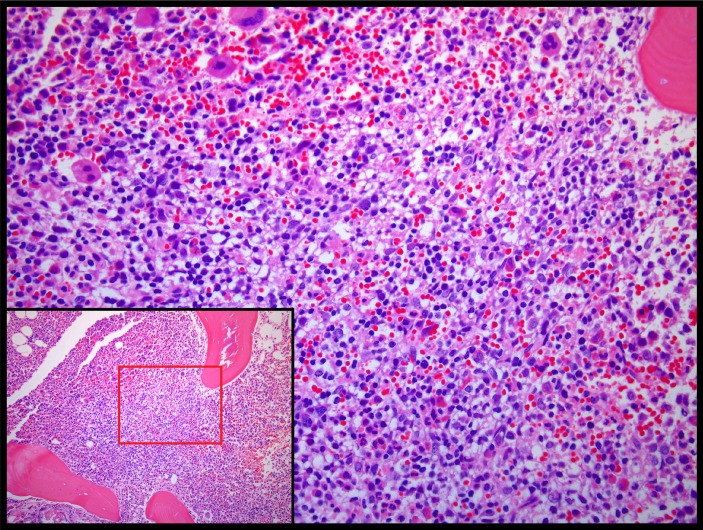
Laryngeal involvement is a rare manifestation of mycosis fungoides (MF), with only nine reported cases of cutaneous T cell lymphoma with laryngeal or vocal cord involvement. Herein, we report the case of a patient with a 7-year history of MF who presented to the emergency department with hoarseness, throat tightness and cough, as well as erythroderma and skin tumours. Laryngoscopy and CT imaging were concerning for lymphomatous involvement of the left false vocal cord. A biopsy was taken of the false vocal cord lesion, which revealed an aberrant immunophenotype consistent with MF. The patient was started on doxorubicin with initial rapid improvement in symptoms. Within 2 months, her respiratory status and skin involvement worsened. Subsequent studies showed bone marrow involvement. The patient expired 4 months after original presentation. This report describes the patient's presentation and clinical course, and reviews the literature on vocal cord and laryngeal involvement of MF.
Keywords: dermatology; ear, nose and throat/otolaryngology; immunology.
© BMJ Publishing Group Ltd (unless otherwise stated in the text of the article) 2017. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical