

Management of thromboembolism-in-transit with pulmonary embolism
- PMID: 28993433
- PMCID: PMC5640568
- DOI: 10.1530/ERP-17-0043
Management of thromboembolism-in-transit with pulmonary embolism
Abstract
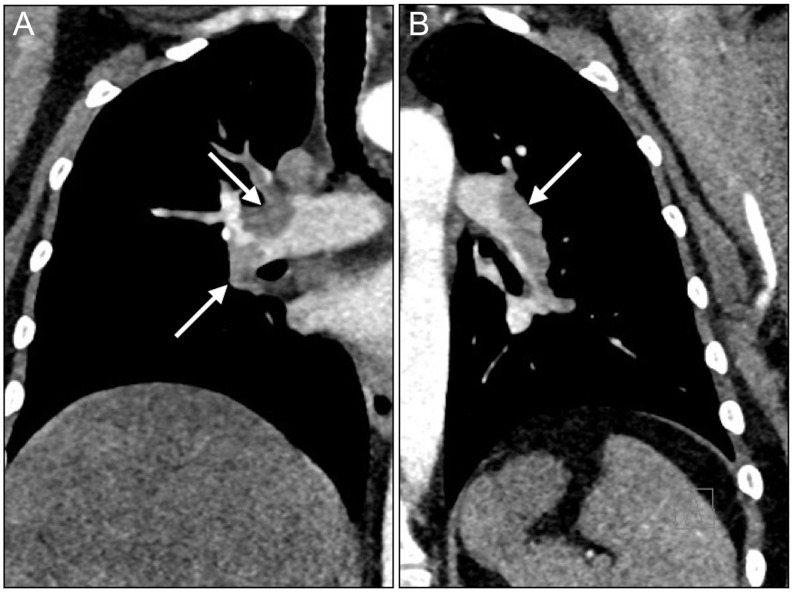
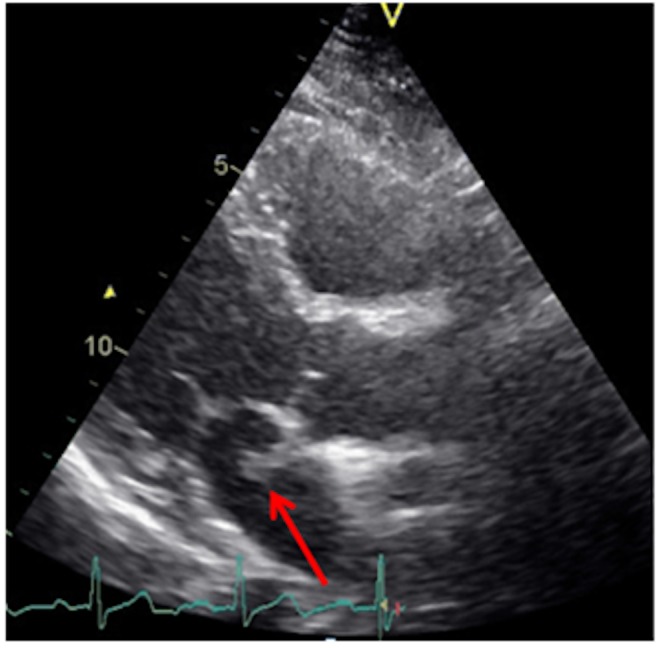
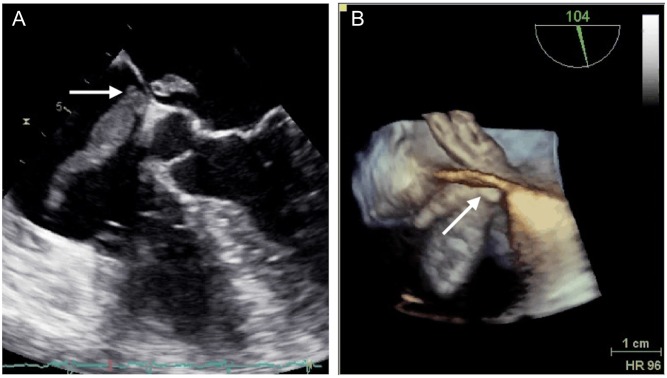
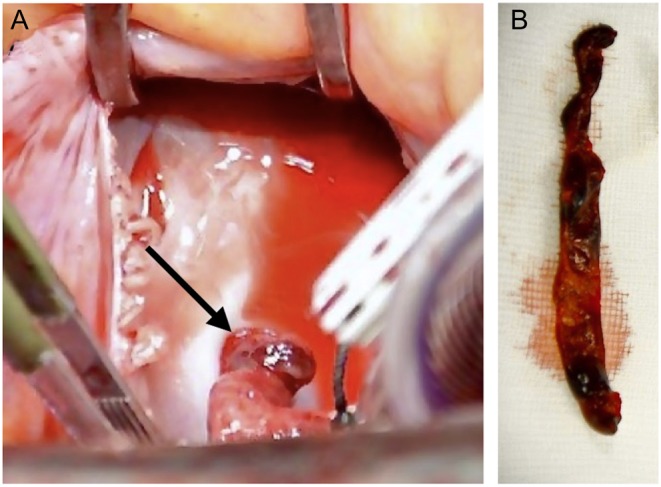
We present a rare complication of deep venous thrombosis with pulmonary embolism that threatened the patient with systemic embolization. A 36-year-old female was referred to the hospital after five days of progressive shortness of breath and chest pain. Preceding onset of symptoms, she had undergone surgery leading to reduced physical activity and had just returned from vacation by a long flight. Investigations with transthoracic and transesophageal echocardiography revealed a thromboembolism-in-transit across a patent foramen ovale. Thoracic CT showed submassive bilateral pulmonary embolism. Hemodynamic parameters were stable. The patient was treated surgically with extraction of the thrombus, closure of the foramen ovale and removal of the bilateral pulmonary emboli. She was discharged after an uneventful hospital stay.
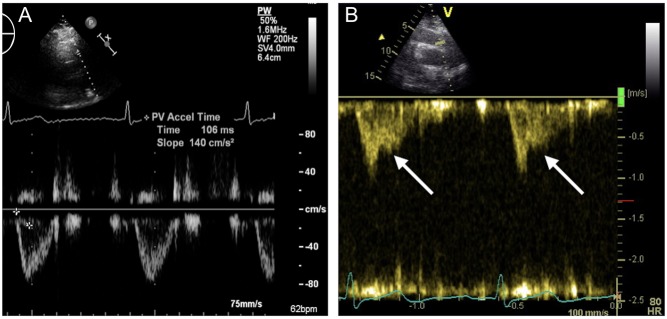
Learning points: Thromboembolism-in-transit across a patent foramen ovale usually occurs in the presence of deep venous thrombosis with pulmonary embolism. The abrupt rise in pulmonary arterial pressure may contribute to the migration of the thrombus across the atrial septum to the systemic circulation.If any abnormal structures are seen in the left atrium by TTE in a patient with pulmonary embolism, a TEE should be performed to rule out an embolus entrapped in a patent foramen ovale.When acute pulmonary hypertension cannot be assessed by conventional methods, additional parameters such as shortened right ventricular outflow tract acceleration time and a mid-systolic notching of the pulse wave Doppler profile in the right ventricular outflow tract may be useful.Mortality is highest during the initial 24 h after onset of chest symptoms; thus, optimal treatment must commence urgently.The choice of treatment in each individual patient must be made after a thorough discussion in a multidisciplinary heart team.
Keywords: patent foramen ovale; pulmonary embolism; surgery; transesophageal echocardiography; transthoracic echocardiography.
© 2017 The authors.
Figures
References
-
- Zamorano JL, Achenbach S, Baumgartner H, Bax JJ, Bueno H, Dean V, Çetin Erol CD, Fagard R, Ferrari R, Hasdai D, et al. 2014. 2014 ESC Guidelines on the diagnosis and management of acute pulmonary embolism: The Task Force for the Diagnosis and Management of Acute Pulmonary Embolism of the European Society of Cardiology (ESC) Endorsed by the European Respiratory Society (ERS). European Heart Journal 35 3033–3073. ( 10.1093/eurheartj/ehu283) - DOI - PubMed
-
- Harjola V-P, Mebazaa A, Čelutkienė J, Bettex D, Bueno H, Chioncel O, Crespo-Leiro MG, Falk V, Filippatos G, Gibbs S, et al. 2016. Contemporary management of acute right ventricular failure: a statement from the Heart Failure Association and the Working Group on Pulmonary Circulation and Right Ventricular Function of the European Society of Cardiology. European Journal of Heart Failure 18 226–241. ( 10.1002/ejhf.478) - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
