

The effect of everolimus on renal angiomyolipoma in pediatric patients with tuberous sclerosis being treated for subependymal giant cell astrocytoma
- PMID: 28993887
- PMCID: PMC5700234
- DOI: 10.1007/s00467-017-3806-1
The effect of everolimus on renal angiomyolipoma in pediatric patients with tuberous sclerosis being treated for subependymal giant cell astrocytoma
Abstract
Background: Patients with tuberous sclerosis complex (TSC) often have multiple TSC-associated hamartomas, particularly in the brain and kidney.
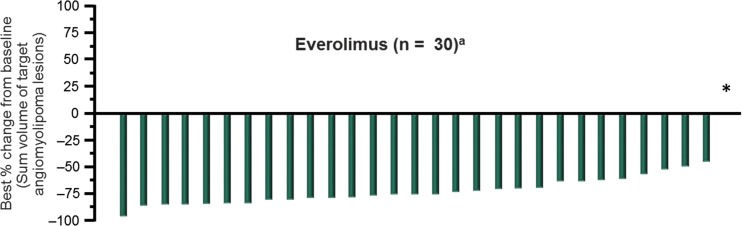
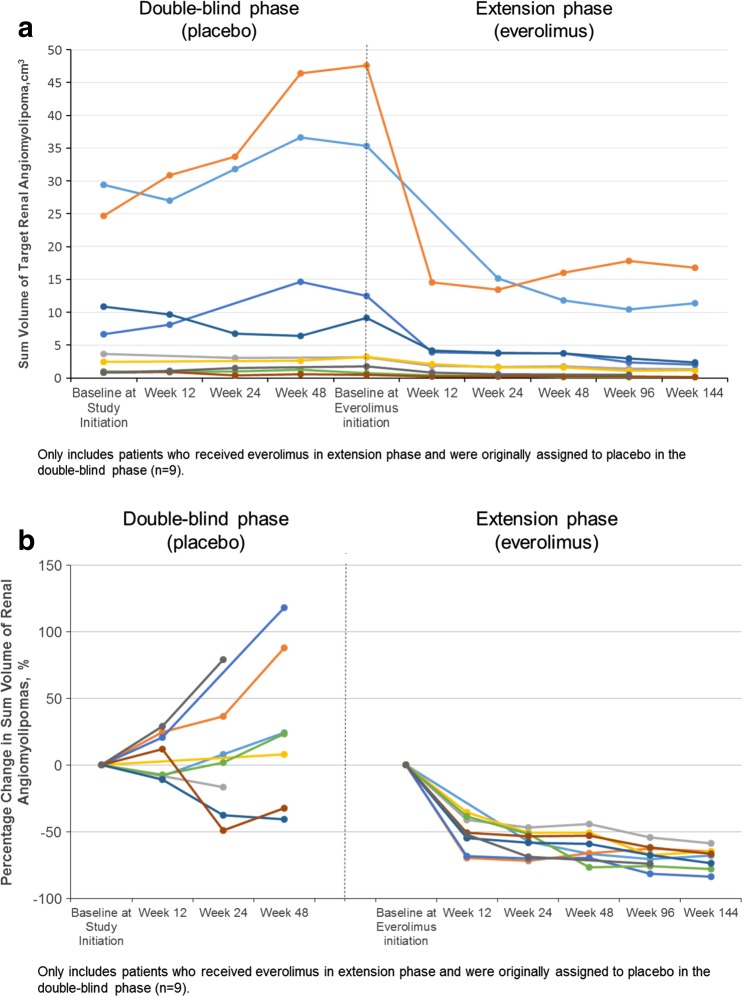
Methods: This was a post hoc analysis of pediatric patients being treated for subependymal giant cell astrocytomas (SEGAs) during the phase 3, randomized, double-blind, placebo-controlled EXIST-1 trial. Patients were initially randomly assigned to receive everolimus 4.5 mg/m2/day (target blood trough 5-15 mg/dl) or placebo and could continue in an open-label extension phase. Angiomyolipoma response rates were analyzed in patients aged <18 years with ≥1 target angiomyolipoma lesion at baseline. Response was defined as the proportion of patients with a ≥50% reduction in the sum volume of target renal angiomyolipomata from baseline, in the absence of new target angiomyolipomata, a >20% increase in kidney volume from nadir, and angiomyolipoma-related bleeding ≥ grade 2. Tolerability was also assessed.
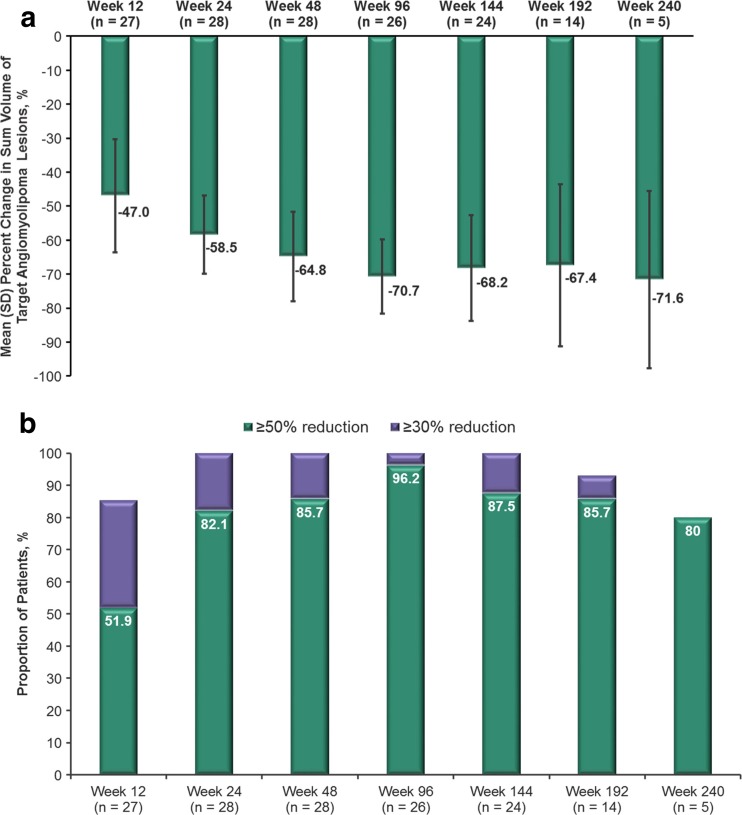
Results: Overall, this analysis included 33 patients. Renal angiomyolipoma response was achieved by 75.8% of patients (95% confidence interval, 57.7-88.9%), with sustained mean reductions in renal angiomyolipoma volume over nearly 4 years of treatment. In addition, most (≥80%) achieved clinically relevant reductions in angiomyolipoma volume (≥50%), beginning at week 24 and continuing for the remainder of the study. Everolimus was generally well tolerated in this subgroup, with most adverse events being grade 1 or 2 in severity.
Conclusions: Although everolimus is currently not indicated for this use, this analysis from EXIST-1 demonstrates its long-term efficacy and safety for the treatment of renal angiomyolipoma in pediatric patients undergoing treatment for TSC-associated SEGA.
Keywords: Angiomyolipoma; Everolimus; Pediatrics; Subependymal giant cell astrocytoma; Tuberous sclerosis complex.
Conflict of interest statement
Disclosures
JJB, DNF, MDF, EB, EMB, SS, and JCK have served as study investigators and received research grants (to their institutions) from Novartis and have served as consultants and/or participated in advisory boards for Novartis. JJB, DNF, MDF, EB, SS, and JCK have received travel honoraria from Novartis. NB and AR are employees of Novartis.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
