

Effect of a high dosage opioid prior authorization policy on prescription opioid use, misuse, and overdose outcomes
- PMID: 29016245
- PMCID: PMC9926935
- DOI: 10.1080/08897077.2017.1389798
Effect of a high dosage opioid prior authorization policy on prescription opioid use, misuse, and overdose outcomes
Abstract
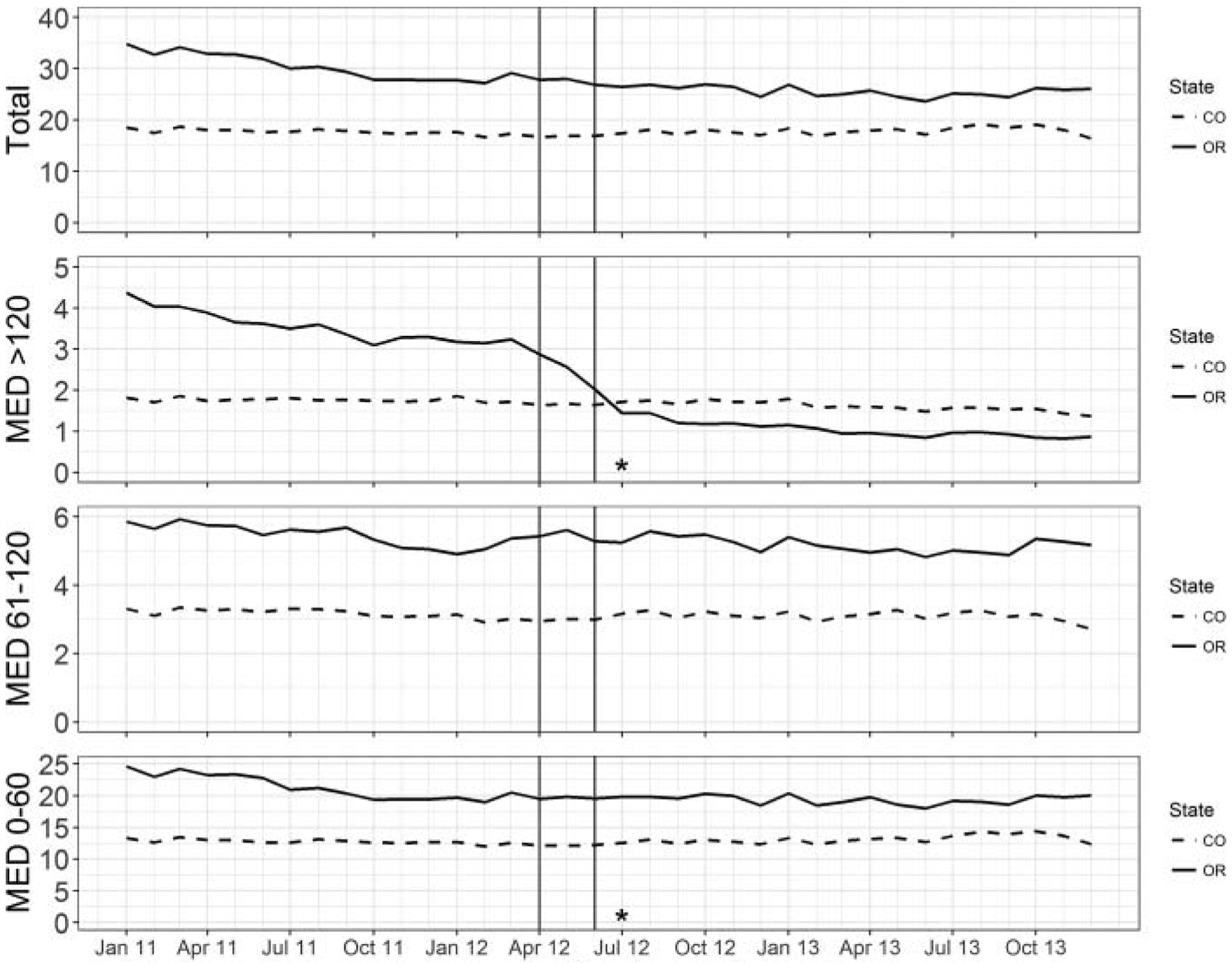
Background: High dosage opioid use is a risk factor for opioid-related overdose commonly cited in guidelines, recommendations, and policies. In 2012, the Oregon Medicaid program developed a prior authorization policy for opioid prescriptions above 120 mg per day morphine equivalent dose (MED). This study aimed to evaluate the effects of that policy on utilization, prescribing patterns, and health outcomes.
Methods: Using administrative claims data from Oregon and a control state (Colorado) between 2011 and 2013, we used difference-in-differences analyses to examine changes in utilization, measures of high risk opioid use, and overdose after introduction of the policy. We also evaluated opioid utilization in a cohort of individuals who were high dosage opioid users before the policy.
Results: Following implementation of Oregon's high dosage policy, the monthly probability of an opioid fill over 120 mg MED declined significantly by 1.7 percentage points (95% confidence interval [CI]; -2.0% to -1.4%), whereas it increased significantly by 1.0 percentage points (95% CI 0.4% to 1.7%) for opioid fills < 61 mg MED. Fills of medications used to treat neuropathic pain also increased by 1.2 percentage points (95% CI 0.7% to 1.8%). The monthly probability of multiple pharmacy use declined by 0.1 percentage points (-0.2% to -0.0) following the prior authorization, but there were no significant changes in ED encounters or hospitalizations for opioid overdose. Among individuals who were using a high dosage opioid before the policy, there was a 20.3 percentage point (95% CI -15.3% to -25.3%) decline in estimated probability of having a high dosage fill after the policy.
Conclusions: Oregon's prior authorization policy was effective at reducing high dosage opioid prescriptions. While multiple pharmacy use also declined, we found no impact on opioid overdose were observed.
Keywords: Medicaid; Opioid; overdose; prior authorization.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
References
-
- Centers for Disease Control and Prevention. Wide-ranging Online Data for Epidemiologic Research (WONDER). Atlanta, GA: Centers for Disease Control and Prevention; 2015.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
