

Randomized trial of two doses of vitamin D3 in preterm infants <32 weeks: Dose impact on achieving desired serum 25(OH)D3 in a NICU population
- PMID: 29016653
- PMCID: PMC5634602
- DOI: 10.1371/journal.pone.0185950
Randomized trial of two doses of vitamin D3 in preterm infants <32 weeks: Dose impact on achieving desired serum 25(OH)D3 in a NICU population
Abstract
Background: Recommendations for vitamin D supplementation for preterm infants span a wide range of doses. Response to vitamin D supplementation and impact on outcomes in preterm infants is not well understood.
Objective: Evaluate serum 25(OH)D3 concentration changes after 4 weeks in response to two different doses of vitamin D3 supplementation in a population of premature infants and quantify the impact on NICU outcomes.
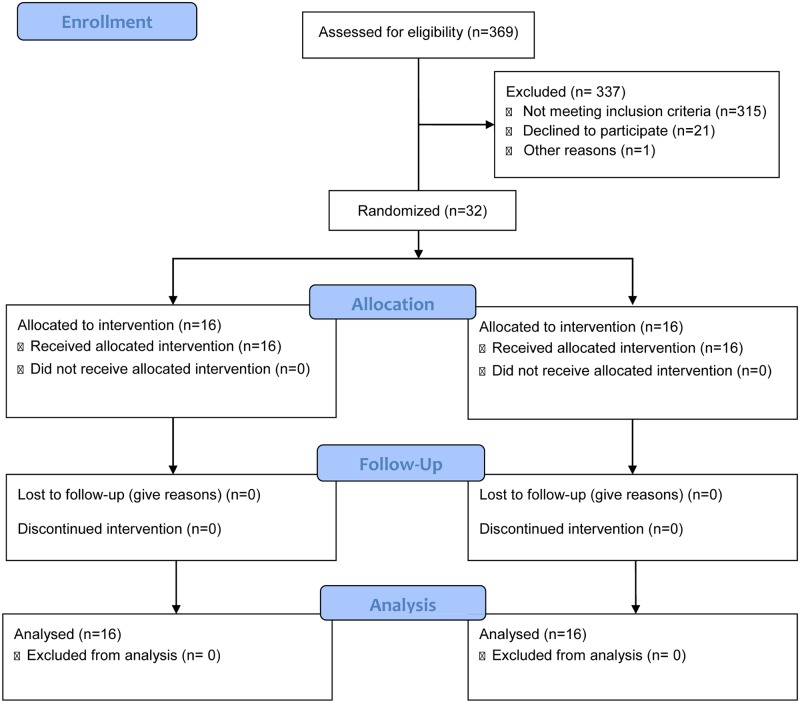
Design: 32 infants born at 24-32 weeks gestation were prospectively randomized to receive 400 or 800 IU/day vitamin D3 supplementation. Serum 25(OH)D3 levels were measured every 4 weeks. The Wilcoxon signed rank test was used to compare serum levels of 25(OH)D3 at 4 weeks and each subsequent time point. A p-value of <0.05 was considered statistically significant.
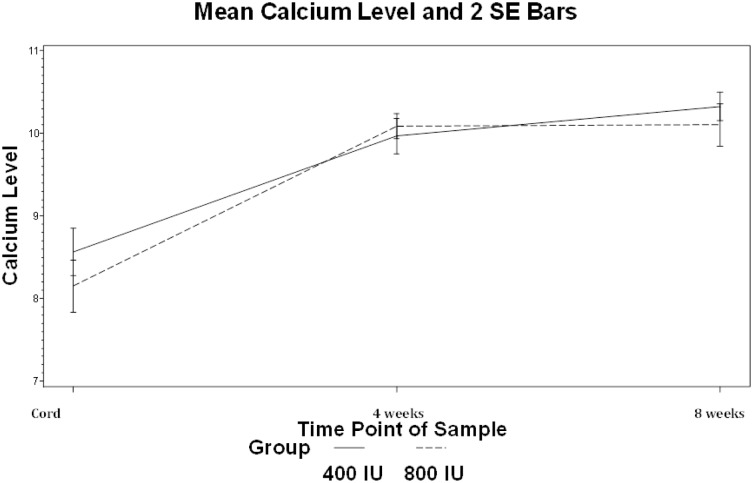
Results: Serum 25(OH)D3 levels at birth were 41.9 and 42.9 nmol/l for infants in the 400 IU group and 800 IU group, respectively (p = 0.86). Cord 25(OH)D3 concentrations significantly correlated with gestational age (r = 0.40, p = 0.04). After 4 weeks of D3 supplementation, median 25(OH)D3 levels increased in both groups (84.6vs. 105.3 nmol/l for 400 vs. 800 IU/day respectively, with significantly more improvement in the higher dose (p = 0.048). Infants in the 400 IU group were significantly more likely to have dual energy x-ray absorptiometry (DEXA) bone density measurements <10 percentile (56% vs 16%, p = 0.04).
Conclusions: Improvement in 25(OH)D3 levels at 4 weeks, bone density, and trends towards improvement in linear growth support consideration of a daily dose of 800 IU of vitamin D for infants <32 weeks cared for in the NICU.
Conflict of interest statement
Figures
References
-
- Stocklin E, Eggersdorfer M. Vitamin D, an essential nutrient with versatile functions in nearly all organs. Int J Vitam Nutr Res. 2013;83(2):92–100. doi: 10.1024/0300-9831/a000151 - DOI - PubMed
-
- Misra M, Pacaud D, Petryk A, Collett-Solberg PF, Kappy M, Drug and Therapeutics Committee of the Lawson Wilkins Pediatric Endocrine Society. Vitamin D deficiency in children and its management: Review of current knowledge and recommendations. Pediatrics. 2008;122(2):398–417. doi: 10.1542/peds.2007-1894 - DOI - PubMed
-
- Priemel M, von Domarus C, Klatte TO, Kessler S, Schlie J, Meier S, et al. Bone mineralization defects and vitamin D deficiency: Histomorphometric analysis of iliac crest bone biopsies and circulating 25-hydroxyvitamin D in 675 patients. J Bone Miner Res. 2010;25(2):305–312. doi: 10.1359/jbmr.090728 - DOI - PubMed
-
- Agostoni C, Buonocore G, Carnielli VP, De Curtis M, Darmaun D, Decsi T, et al. Enteral nutrient supply for preterm infants: Commentary from the European Society of Paediatric Gastroenterology, Hepatology and Nutrition Committee on Nutrition. J Pediatr Gastroenterol Nutr. 2010;50(1):85–91. doi: 10.1097/MPG.0b013e3181adaee0 - DOI - PubMed
-
- Wagner CL, Greer FR, American Academy of Pediatrics Section on Breastfeeding, American Academy of Pediatrics Committee on Nutrition. Prevention of rickets and vitamin D deficiency in infants, children, and adolescents. Pediatrics. 2008;122(5):1142–1152. doi: 10.1542/peds.2008-1862 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
