

Efficacy of azole therapy for tegumentary leishmaniasis: A systematic review and meta-analysis
- PMID: 29016694
- PMCID: PMC5633178
- DOI: 10.1371/journal.pone.0186117
Efficacy of azole therapy for tegumentary leishmaniasis: A systematic review and meta-analysis
Abstract
Background: Several controlled and uncontrolled studies addressing azole antifungal drugs for cutaneous and mucosal leishmaniasis have been published with inconclusive results. We conducted a systematic literature review of studies evaluating the efficacy and toxicity associated with azole therapy for tegumentary leishmaniasis.
Methodology: PRISMA guidelines for systematic reviews and the Cochrane manual were followed, and the review methodology was registered (PROSPERO; CRD42016048668). Sources included the EMBASE, Web of Science, MEDLINE, LILACS, and IBECS databases along with a manual search of references from evaluated studies. Additional resources such as Google Scholar and clinicaltrials.gov were also searched. We included all studies reporting cure rate after cutaneous or mucosal leishmaniasis treatment with systemic azole drugs, regardless of their design. R software was used to estimate global rates of success and adverse events with each drug. The main outcome of interest was clinical cure, defined as complete re-epithelialization of all lesions.
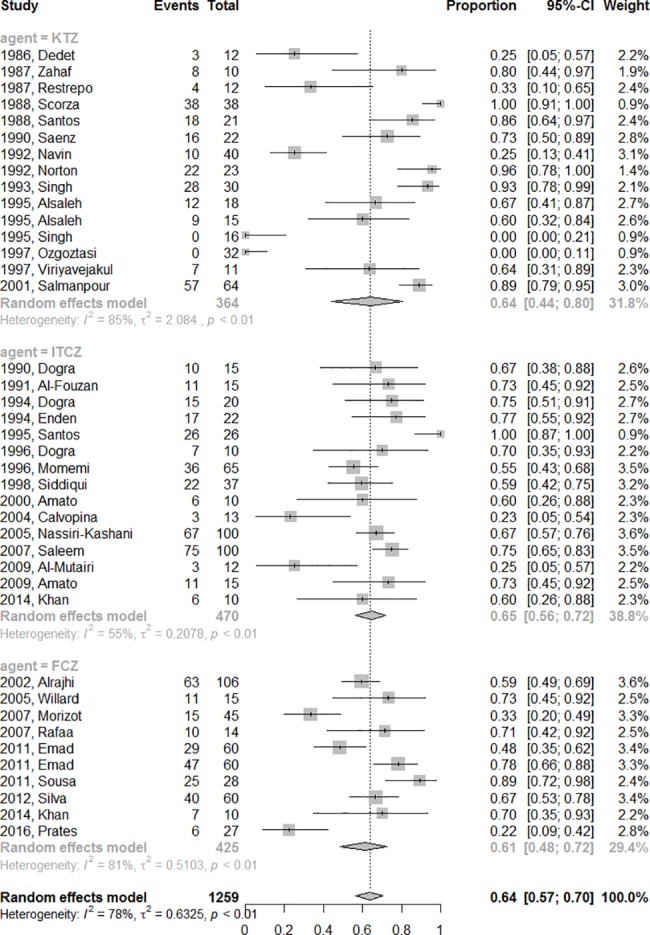
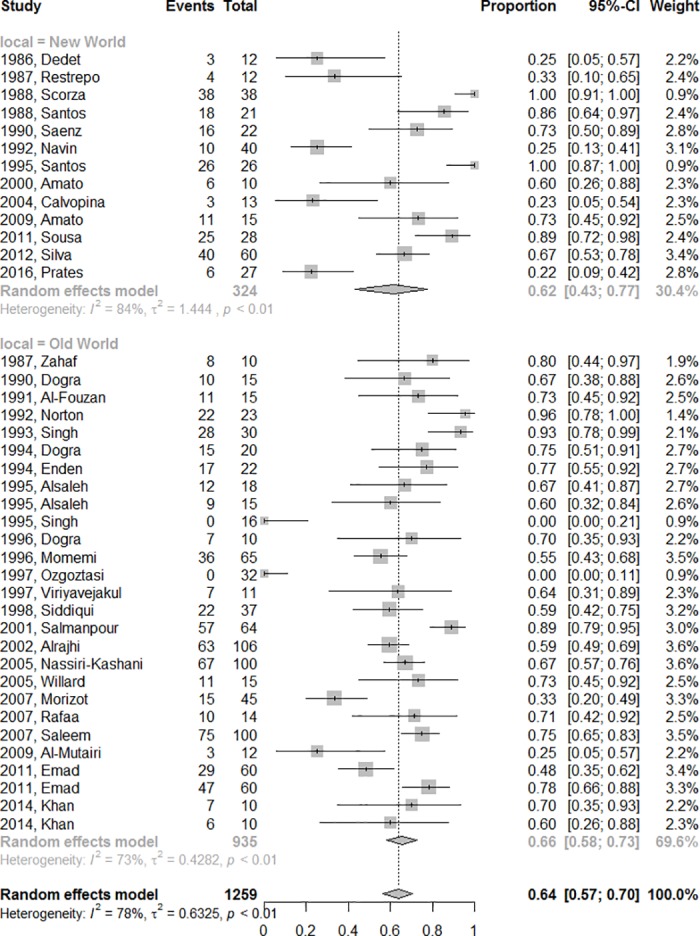
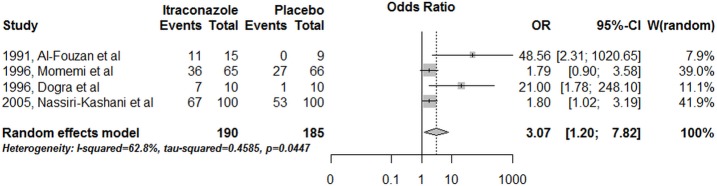
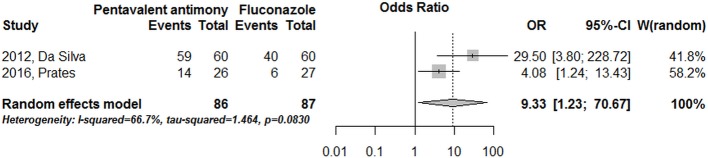
Results: A total of 37 studies involving 1259 patients that reported outcomes after fluconazole (9), ketoconazole (14) and itraconazole (15) treatments were included. Only 14 (38%) were randomized controlled trials (RCT). The pooled azole final efficacy rate was 64% (CI95%: 57-70%) for all studies and 60% (CI95%: 50-70%) (p = 0.41) if only RCTs studies were considered. Twenty-four studies were conducted in the Old World and 13 studies in the Americas. The final efficacy rate according to New and Old World were 62% (CI95%: 43-77%) and 66% (CI95%: 58-73%), respectively. The final efficacy rate of azoles according to species were 89% (CI95%: 50-98%) for L. mexicana; 88% for L. infantum (CI95%: 27-99%); 80% for L. donovani; 53% (CI95%: 29-76%) for L. major; 49% for L. braziliensis (CI95%: 21-78%); and 15% (CI95%: 1-84%) for L. tropica. The cure rates were similar among the fluconazole, ketoconazole and itraconazole group arms (p = 0.89), specifically 61% (CI95%: 48-72%), 64% (CI95%: 44-80%) 65% (CI95%: 56-72%), respectively. Adverse events during fluconazole, itraconazole and ketoconazole therapy were reported in 7% (CI95%: 3-14%), 12% (CI95% 8-19%) and 13% (CI95%: 6-29%) of treated patients, respectively, without difference among them (p = 0.35). This systematic review included studies with small samples and both non-comparative and non-randomized studies and the main limitation was the low quality of the available studies.
Conclusions: Available evidence suggests that fluconazole, ketoconazole and itraconazole have similar and modest efficacy rates for tegumentary leishmaniasis treatment. There is insufficient evidence to support the exclusive use of azole therapy as a single agent for leishmaniasis treatment.
Conflict of interest statement
Figures


References
-
- Alvar J, Vélez1 ID, Bern C, Herrero M, Desjeux P, Cano J, et al. The WHO Leishmaniasis Control Team. Leishmaniasis Worldwide and Global Estimates of Its Incidence. PLoS One. 2012; 7(5), e35671 Epub 2012/05/31. doi: 10.1371/journal.pone.0035671 - DOI - PMC - PubMed
-
- Gurel MS, Yanik M, Simsek Z, Kati M, Karaman A. Quality of life instrument for Turkish people with skin diseases. Int J Dermatol. 2015; 44(11):933–8 doi: 10.1111/j.1365-4632.2004.02225.x - DOI - PubMed
-
- Kassi M, Kassi M, Afghan AK, Rehman R, Kasi PM. Marring Leishmaniasis: The Stigmatization and the Impact of Cutaneous Leishmaniasis in Pakistan and Afghanistan. PLoS Negl Trop Dis. 2008; 2(10):e259 Epub 2008/10/29. doi: 10.1371/journal.pntd.0000259 - DOI - PMC - PubMed
-
- Chahed MK, Bellali H, Jemaa SB, Belaj T. Pscychological and Psicosocial consequences of zoonotic Cutaneous Leishmaniasis among Women in Tunisia: Preliminary Findings from an exploratory Study. PLoS Negl Trop Dis. 2016; October 27;10(10):e0005090 eCollection 2016. doi: 10.1371/journal.pntd.0005090 - DOI - PMC - PubMed
-
- Khatami A, Firooz A, Gorouhi F, Dowlati Y. Treatment of acute Old World cutaneous leishmaniasis: a systematic review of the randomized controlled trials. J Am Acad Dermatol. 2007; 57(2):335.e1–29. Epub 2007/03/06. doi: 10.1016/j.jaad.2007.01.016 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
