

Cardiac troponins: from myocardial infarction to chronic disease
- PMID: 29016754
- PMCID: PMC5852618
- DOI: 10.1093/cvr/cvx183
Cardiac troponins: from myocardial infarction to chronic disease
Abstract
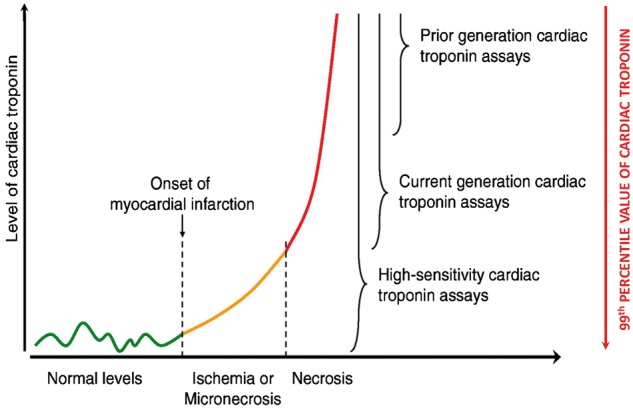
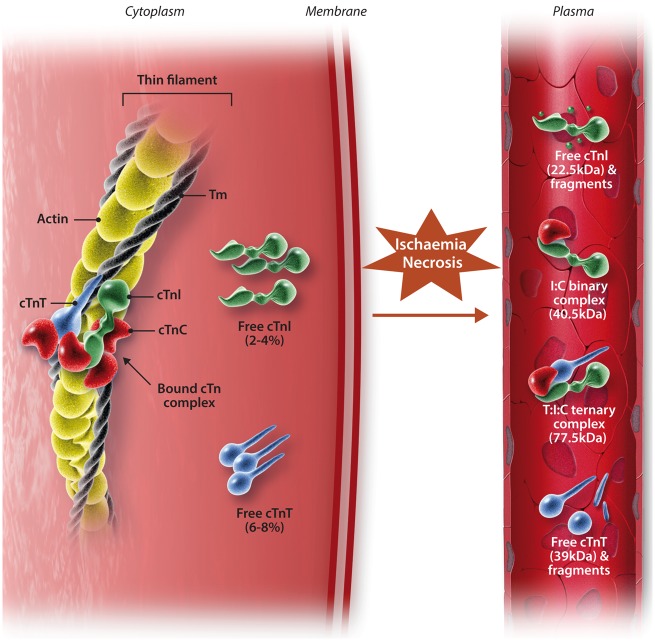
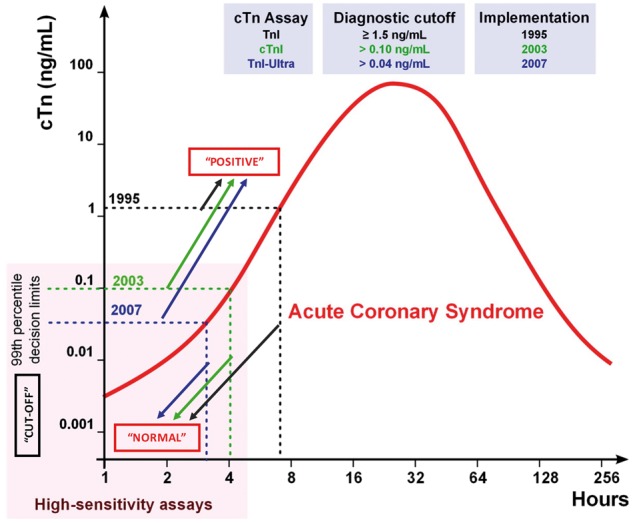
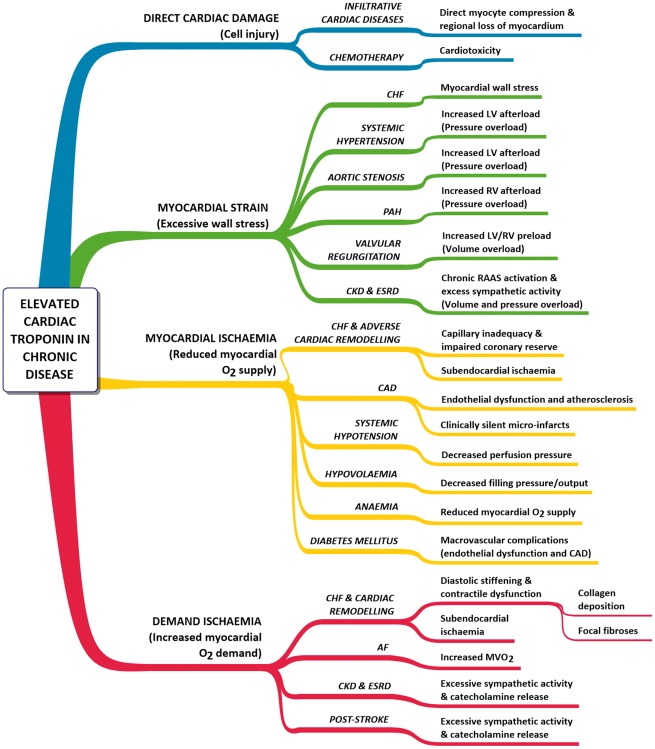
Elucidation of the physiologically distinct subunits of troponin in 1973 greatly facilitated our understanding of cardiac contraction. Although troponins are expressed in both skeletal and cardiac muscle, there are isoforms of troponin I/T expressed selectively in the heart. By exploiting cardiac-restricted epitopes within these proteins, one of the most successful diagnostic tests to date has been developed: cardiac troponin (cTn) assays. For the past decade, cTn has been regarded as the gold-standard marker for acute myocardial necrosis: the pathological hallmark of acute myocardial infarction (AMI). Whilst cTn is the cornerstone for ruling-out AMI in patients presenting with a suspected acute coronary syndrome (ACS), elevated cTn is frequently observed in those without clinical signs indicative of AMI, often reflecting myocardial injury of 'unknown origin'. cTn is commonly elevated in acute non-ACS conditions, as well as in chronic diseases. It is unclear why these elevations occur; yet they cannot be ignored as cTn levels in chronically unwell patients are directly correlated to prognosis. Paradoxically, improvements in assay sensitivity have meant more differential diagnoses have to be considered due to decreased specificity, since cTn is now more easily detected in these non-ACS conditions. It is important to be aware cTn is highly specific for myocardial injury, which could be attributable to a myriad of underlying causes, emphasizing the notion that cTn is an organ-specific, not disease-specific biomarker. Furthermore, the ability to detect increased cTn using high-sensitivity assays following extreme exercise is disconcerting. It has been suggested troponin release can occur without cardiomyocyte necrosis, contradicting conventional dogma, emphasizing a need to understand the mechanisms of such release. This review discusses basic troponin biology, the physiology behind its detection in serum, its use in the diagnosis of AMI, and some key concepts and experimental evidence as to why cTn can be elevated in chronic diseases.
Keywords: Biomarker; Cardiac troponin; Chronic disease; Prognosis; Release mechanism.
© The Author 2017. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
-
- Greaser ML, Gergely J.. Purification and properties of the components from troponin. J Biol Chem 1973;248:2125–2133. - PubMed
-
- Thygesen K, Alpert JS, Jaffe AS, Simoons ML, Chaitman BR, White HD, Thygesen K, Alpert JS, White HD, Jaffe AS, Katus HA, Apple FS, Lindahl B, Morrow DA, Chaitman BA, Clemmensen PM, Johanson P, Hod H, Underwood R, Bax JJ, Bonow RO, Pinto F, Gibbons RJ, Fox KA, Atar D, Newby LK, Galvani M, Hamm CW, Uretsky BF, Steg PG, Wijns W, Bassand JP, Menasche P, Ravkilde J, Ohman EM, Antman EM, Wallentin LC, Armstrong PW, Simoons ML, Januzzi JL, Nieminen MS, Gheorghiade M, Filippatos G, Luepker RV, Fortmann SP, Rosamond WD, Levy D, Wood D, Smith SC, Hu D, Lopez-Sendon JL, Robertson RM, Weaver D, Tendera M, Bove AA, Parkhomenko AN, Vasilieva EJ, Mendis S.. Joint ESC/ACCF/AHA/WHF Task Force for the Universal Definition of Myocardial Infarction. Third universal definition of myocardial infarction. Eur Heart J 2012;33:2551–2567.
-
- Roffi M, Patrono C, Collet J-P, Mueller C, Valgimigli M, Andreotti F, Bax JJ, Borger MA, Brotons C, Chew DP, Gencer B, Hasenfuss G, Kjeldsen K, Lancellotti P, Landmesser U, Mehilli J, Mukherjee D, Storey RF, Windecker S, Baumgartner H, Gaemperli O, Achenbach S, Agewall S, Badimon L, Baigent C, Bueno H, Bugiardini R, Carerj S, Casselman F, Cuisset T, Erol Ç, Fitzsimons D, Halle M, Hamm C, Hildick-Smith D, Huber K, Iliodromitis E, James S, Lewis BS, Lip GYH, Piepoli MF, Richter D, Rosemann T, Sechtem U, Steg PG, Vrints C, Luis Zamorano J.. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur Heart J 2016;37:267–315. - PubMed
-
- Giannitsis E, Katus HA.. Cardiac troponin level elevations not related to acute coronary syndromes. Nat Rev Cardiol 2013;10:623–634. - PubMed
-
- Tobacman LS. Thin filament-mediated regulation of cardiac contraction. Annu Rev Physiol 1996;58:447–481. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
