

Sex differences in outcomes of primary prevention implantable cardioverter-defibrillator therapy: combined registry data from eleven European countries
- PMID: 29016784
- PMCID: PMC5982785
- DOI: 10.1093/europace/eux176
Sex differences in outcomes of primary prevention implantable cardioverter-defibrillator therapy: combined registry data from eleven European countries
Erratum in
-
Corrigendum.Europace. 2018 Jun 1;20(6):970. doi: 10.1093/europace/eux348. Europace. 2018. PMID: 29126232 Free PMC article. No abstract available.
Abstract
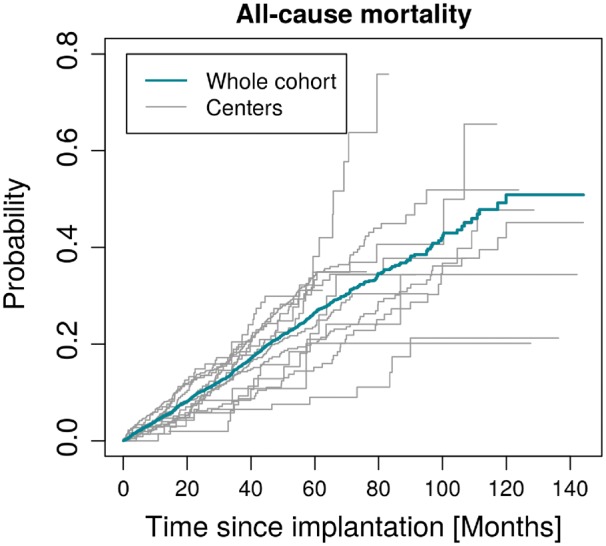
Aims: Therapy with an implantable cardioverter defibrillator (ICD) is established for the prevention of sudden cardiac death (SCD) in high risk patients. We aimed to determine the effectiveness of primary prevention ICD therapy by analysing registry data from 14 centres in 11 European countries compiled between 2002 and 2014, with emphasis on outcomes in women who have been underrepresented in all trials.
Methods and results: Retrospective data of 14 local registries of primary prevention ICD implantations between 2002 and 2014 were compiled in a central database. Predefined primary outcome measures were overall mortality and first appropriate and first inappropriate shocks. A multivariable model enforcing a common hazard ratio for sex category across the centres, but allowing for centre-specific baseline hazards and centre specific effects of other covariates, was adjusted for age, the presence of ischaemic cardiomyopathy or a CRT-D, and left ventricular ejection fraction ≤25%. Of the 5033 patients, 957 (19%) were women. During a median follow-up of 33 months (IQR 16-55 months) 129 women (13%) and 807 men (20%) died (HR 0.65; 95% CI: [0.53, 0.79], P-value < 0.0001). An appropriate ICD shock occurred in 66 women (8%) and 514 men (14%; HR 0.61; 95% CI: 0.47-0.79; P = 0.0002).
Conclusion: Our retrospective analysis of 14 local registries in 11 European countries demonstrates that fewer women than men undergo ICD implantation for primary prevention. After multivariate adjustment, women have a significantly lower mortality and receive fewer appropriate ICD shocks.
Figures





References
-
- Moss AJ, Zareba W, Hall WJ, Klein H, Wilber DJ, Cannom DS. et al. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med 2002;346:877–83. - PubMed
-
- Bardy GH, Lee KL, Mark DB, Poole JE, Packer DL, Boineau R. et al. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. N Engl J Med 2005;352:225–37. - PubMed
-
- Koller MT, Schaer B, Wolbers M, Sticherling C, Bucher HC, Osswald S.. Death without prior appropriate implantable cardioverter-defibrillator therapy: a competing risk study. Circulation 2008;117:1918–26. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
