

Posterior fossa syndrome and long-term neuropsychological outcomes among children treated for medulloblastoma on a multi-institutional, prospective study
- PMID: 29016818
- PMCID: PMC5716082
- DOI: 10.1093/neuonc/nox135
Posterior fossa syndrome and long-term neuropsychological outcomes among children treated for medulloblastoma on a multi-institutional, prospective study
Abstract
Background: Patients treated for medulloblastoma who experience posterior fossa syndrome (PFS) demonstrate increased risk for neurocognitive impairment at one year post diagnosis. The aim of the study was to examine longitudinal trajectories of neuropsychological outcomes in patients who experienced PFS compared with patients who did not.
Methods: Participants were 36 patients (22 males) who experienced PFS and 36 comparison patients (21 males) who were matched on age at diagnosis and treatment exposure but did not experience PFS. All patients underwent serial evaluation of neurocognitive functioning spanning 1 to 5 years post diagnosis.
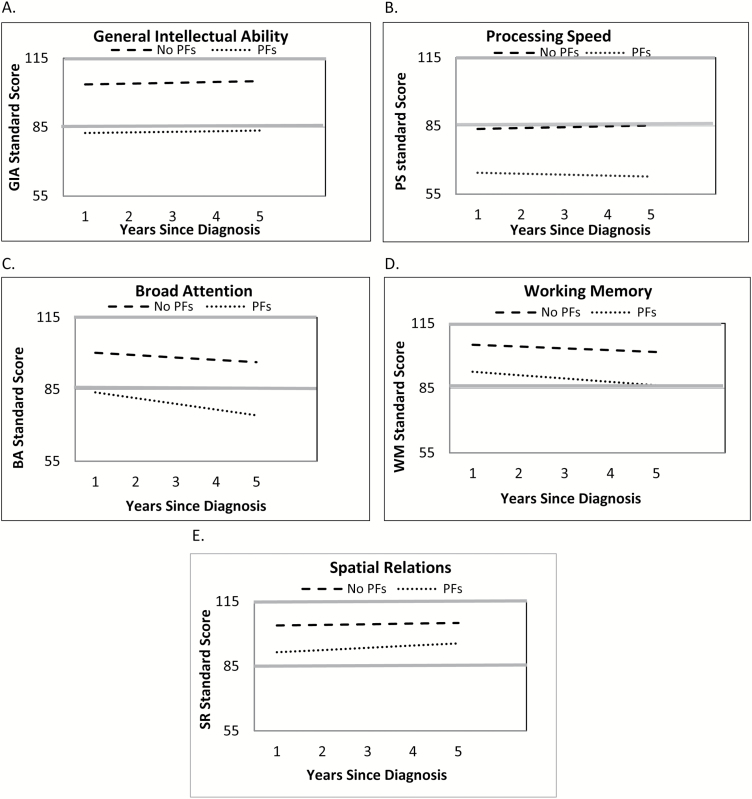
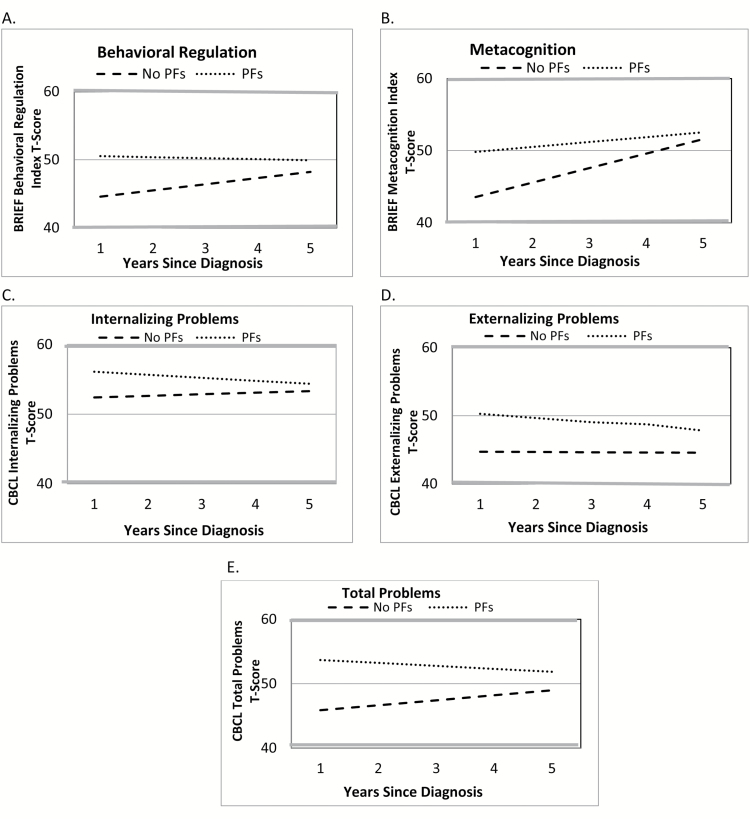
Results: The PFS group demonstrated lower estimated mean scores at 1, 3, and 5 years post diagnosis on measures of general intellectual ability, processing speed, broad attention, working memory, and spatial relations compared with the non-PFS group. The PFS group exhibited estimated mean scores that were at least one standard deviation below the mean for intellectual ability, processing speed, and broad attention across all time points and for working memory by 5 years post diagnosis. Processing speed was stable over time. Attention and working memory declined over time. Despite some change over time, caregiver ratings of executive function and behavior problem symptoms remained within the average range.
Conclusion: Compared with patients who do not experience PFS, patients who experience PFS exhibit greater neurocognitive impairment, show little recovery over time, and decline further in some domains. Findings highlight the particularly high risk for long-term neurocognitive problems in patients who experience PFS and the need for close follow-up and intervention.
Keywords: brain tumor; medulloblastoma; neuropsychological outcomes; posterior fossa syndrome.
© The Author(s) 2017. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com
Figures
References
-
- Gurney JG, Severson RK, Davis S, Robison LL. Incidence of cancer in children in the United States. Sex-, race-, and 1-year age-specific rates by histologic type. Cancer. 1995;75(8):2186–2195. - PubMed
-
- Gajjar A, Chintagumpala M, Ashley D et al. Risk-adapted craniospinal radiotherapy followed by high-dose chemotherapy and stem-cell rescue in children with newly diagnosed medulloblastoma (St Jude Medulloblastoma-96): long-term results from a prospective, multicentre trial. Lancet Oncol. 2006;7(10):813–820. - PubMed
-
- Zeltzer PM, Boyett JM, Finlay JL et al. Metastasis stage, adjuvant treatment, and residual tumor are prognostic factors for medulloblastoma in children: conclusions from the Children’s Cancer Group 921 randomized phase III study. J Clin Oncol. 1999;17(3):832–845. - PubMed
-
- De Smet HJ, Baillieux H, Catsman-Berrevoets C, De Deyn PP, Mariën P, Paquier PF. Postoperative motor speech production in children with the syndrome of ‘cerebellar’ mutism and subsequent dysarthria: a critical review of the literature. Eur J Paediatr Neurol. 2007;11(4):193–207. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
