

Clinical characteristics associated with postoperative seizure control in adult low-grade gliomas: a systematic review and meta-analysis
- PMID: 29016869
- PMCID: PMC5817956
- DOI: 10.1093/neuonc/nox130
Clinical characteristics associated with postoperative seizure control in adult low-grade gliomas: a systematic review and meta-analysis
Abstract
Background: Epilepsy is the most common symptom in patients with supratentorial low-grade gliomas (LGGs), which adversely affects the patient's quality of life. Poor seizure control with anti-epileptic therapy is an indication for surgery in these patients. Recent studies have sought to identify predictors of postoperative seizure control after surgical resection of LGG; gross total resection was shown to be a significant predictor in this respect. However, the prognostic value of other factors is not clear.
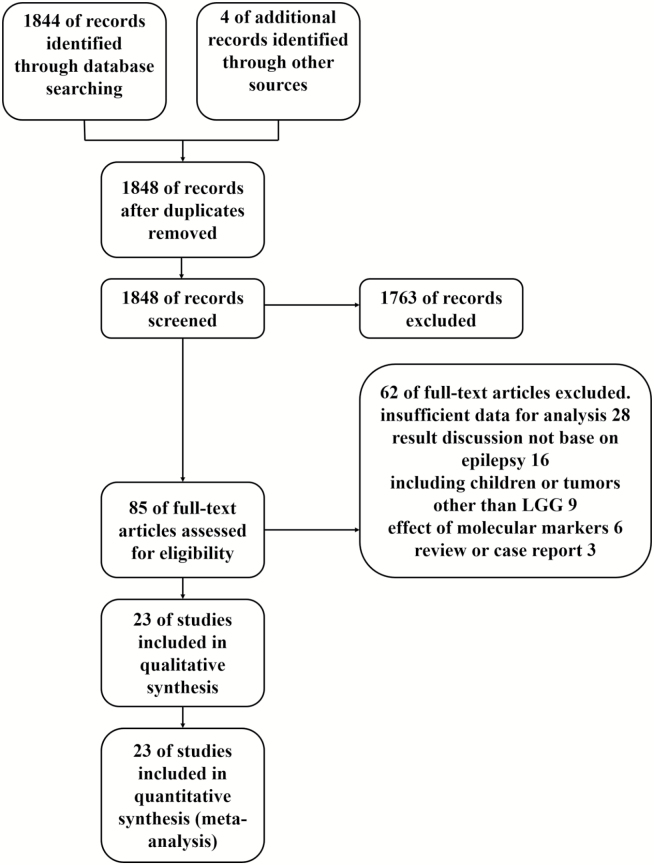
Methods: We performed a systematic review and meta-analysis of 23 studies with a combined study population of 2641 patients with LGG, in order to identify potential factors associated with favorable postoperative seizure control. Data were extracted on age and sex of patient, tumor location, tumor histology, type of seizure, seizure duration, extent of resection, and imaging characteristics.
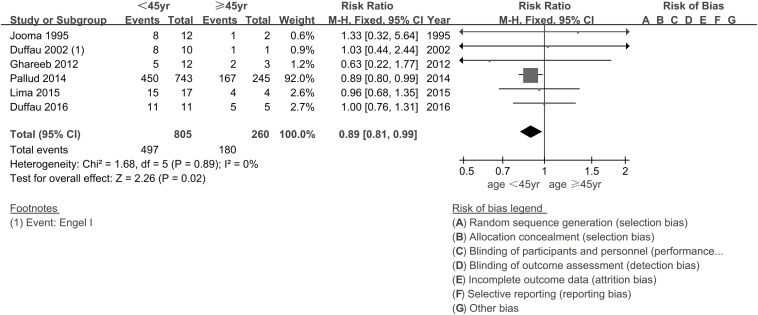
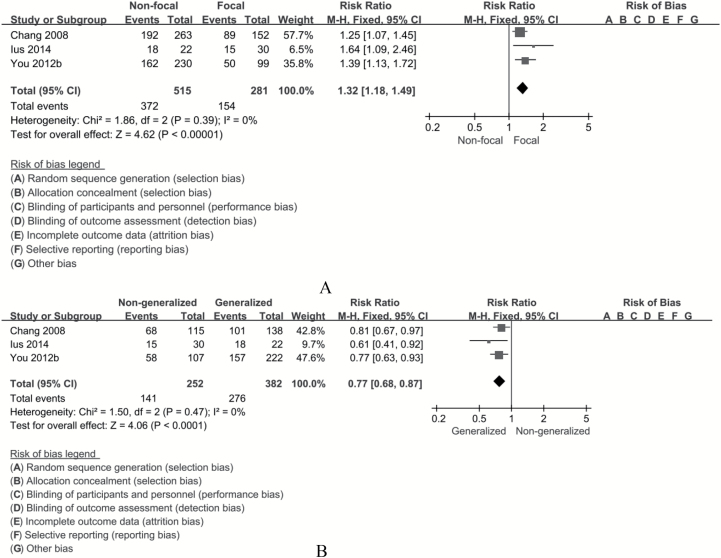
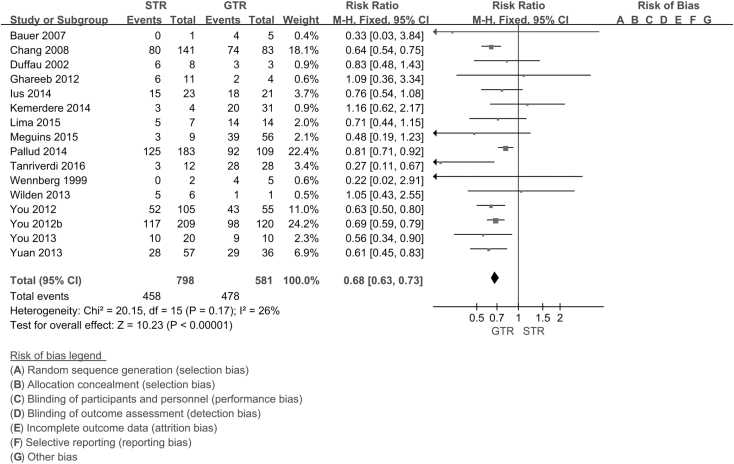
Results: Patients ≥45 years of age achieved better postoperative seizure control (risk ratio [RR], 0.89; 95% CI, 0.81-0.99). Focal seizures were associated with poor seizure control (RR, 1.32; 95% CI, 1.18-1.49) compared with generalized seizures (RR, 0.77; 95% CI, 0.68-0.87). Prolonged history of seizures (≥1 y) had a negative impact on postoperative seizure control (RR, 1.22; 95% CI, 1.10-1.34). Gross total resection was superior to subtotal resection with respect to postoperative seizure control (RR, 0.68; 95% CI, 0.63-0.73).
Conclusions: This systematic review and meta-analysis identified predictors of postoperative seizure control in patients undergoing surgical resection of LGGs. Our results provide a reference for clinical treatment of LGG-related epilepsy.
Published by Oxford University Press on behalf of the Society for Neuro-Oncology 2017. This work is written by (a) US Government employee(s) and is in the public domain in the US.
Figures
References
-
- Louis DN, Perry A, Reifenberger G et al. The 2016 World Health Organization classification of tumors of the central nervous system: a summary. Acta Neuropathol. 2016;131(6):803–820. - PubMed
-
- Lima GL, Duffau H. Is there a risk of seizures in “preventive” awake surgery for incidental diffuse low-grade gliomas?J Neurosurg. 2015;122(6):1397–1405. - PubMed
-
- Duffau H, Capelle L, Lopes M, Bitar A, Sichez JP, van Effenterre R. Medically intractable epilepsy from insular low-grade gliomas: improvement after an extended lesionectomy. Acta Neurochir (Wien). 2002;144(6):563–572; discussion 572. - PubMed
-
- Bartolomei JC, Christopher S, Vives K, Spencer DD, Piepmeier JM. Low-grade gliomas of chronic epilepsy: a distinct clinical and pathological entity. J Neurooncol. 1997;34(1):79–84. - PubMed
-
- Berger MS, Ghatan S, Haglund MM, Dobbins J, Ojemann GA. Low-grade gliomas associated with intractable epilepsy: seizure outcome utilizing electrocorticography during tumor resection. J Neurosurg. 1993;79(1):62–69. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
