

Incremental value of biomarker combinations to predict progression of mild cognitive impairment to Alzheimer's dementia
- PMID: 29017593
- PMCID: PMC5634868
- DOI: 10.1186/s13195-017-0301-7
Incremental value of biomarker combinations to predict progression of mild cognitive impairment to Alzheimer's dementia
Abstract
Background: The progression of mild cognitive impairment (MCI) to Alzheimer's disease (AD) dementia can be predicted by cognitive, neuroimaging, and cerebrospinal fluid (CSF) markers. Since most biomarkers reveal complementary information, a combination of biomarkers may increase the predictive power. We investigated which combination of the Mini-Mental State Examination (MMSE), Clinical Dementia Rating (CDR)-sum-of-boxes, the word list delayed free recall from the Consortium to Establish a Registry of Dementia (CERAD) test battery, hippocampal volume (HCV), amyloid-beta1-42 (Aβ42), amyloid-beta1-40 (Aβ40) levels, the ratio of Aβ42/Aβ40, phosphorylated tau, and total tau (t-Tau) levels in the CSF best predicted a short-term conversion from MCI to AD dementia.
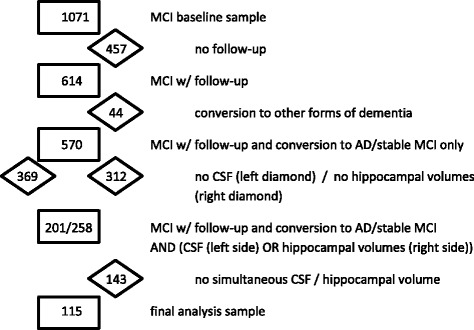
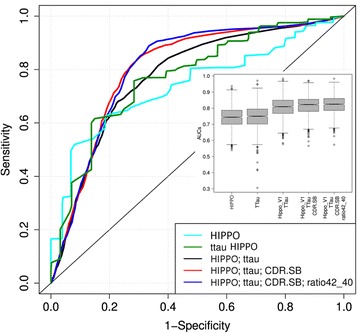
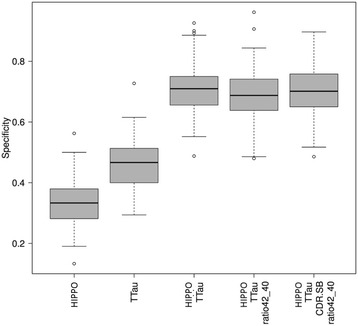
Methods: We used 115 complete datasets from MCI patients of the "Dementia Competence Network", a German multicenter cohort study with annual follow-up up to 3 years. MCI was broadly defined to include amnestic and nonamnestic syndromes. Variables known to predict progression in MCI patients were selected a priori. Nine individual predictors were compared by receiver operating characteristic (ROC) curve analysis. ROC curves of the five best two-, three-, and four-parameter combinations were analyzed for significant superiority by a bootstrapping wrapper around a support vector machine with linear kernel. The incremental value of combinations was tested for statistical significance by comparing the specificities of the different classifiers at a given sensitivity of 85%.
Results: Out of 115 subjects, 28 (24.3%) with MCI progressed to AD dementia within a mean follow-up period of 25.5 months. At baseline, MCI-AD patients were no different from stable MCI in age and gender distribution, but had lower educational attainment. All single biomarkers were significantly different between the two groups at baseline. ROC curves of the individual predictors gave areas under the curve (AUC) between 0.66 and 0.77, and all single predictors were statistically superior to Aβ40. The AUC of the two-parameter combinations ranged from 0.77 to 0.81. The three-parameter combinations ranged from AUC 0.80-0.83, and the four-parameter combination from AUC 0.81-0.82. None of the predictor combinations was significantly superior to the two best single predictors (HCV and t-Tau). When maximizing the AUC differences by fixing sensitivity at 85%, the two- to four-parameter combinations were superior to HCV alone.
Conclusion: A combination of two biomarkers of neurodegeneration (e.g., HCV and t-Tau) is not superior over the single parameters in identifying patients with MCI who are most likely to progress to AD dementia, although there is a gradual increase in the statistical measures across increasing biomarker combinations. This may have implications for clinical diagnosis and for selecting subjects for participation in clinical trials.
Keywords: Alzheimer’s dementia; Amyloid-beta 42; Biomarkers; Hippocampal volume; Mild cognitive impairment; Phospho-tau; Prediction; Tau.
Conflict of interest statement
Authors’ information
Not applicable.
Ethical approval and consent to participate
The DCN study was approved by the Ethics Review Board of the Medical Faculty of the University of Erlangen (coordinating center) and by the Ethics Committees at each individual recruiting site. These were the Ethics Committees of the Medical Faculties of the Universities of Heidelberg (Faculty Mannheim and Faculty Heidelberg), Charité Berlin, Göttingen, Munich (LMU) and Munich (TU), Leipzig, Hamburg, Bonn, Düsseldorf, Freiburg, and Frankfurt/Main. The study was conducted in accordance with the Declaration of Helsinki. All patients gave written informed consent to participate at the point of recruitment to the study.
Consent for publication
All authors have approved the manuscript for submission and gave consent for publication.
Competing interests
LF has received payment for consultancy, expert testimony, honorarium, or traveling support from AstraZeneca, Eisai, Eli Lilly, GE Healthcare, Janssen-Cilag, Lundbeck, Merz Pharma, Novartis, Pfizer, and Schering-Plough, and Apotex Inc., and has received a research grant from Novartis, Pfizer paid to his institution. OP is on scientific advisory boards for Roche, Kyowa Kirin, Novartis, Lilly, and Piramal. He has received funding for travel or speaker honoraria from GSK, Nutricia, and Merck Serono. He has acted as a consultant for Affiris and Roche. He has received research support from Affiris, Piramal, BMS, Eli Lilly, Pfizer, Servier, TRX Pharmaceuticals, Lundbeck, and Genentech. FJ has received consultation board honoraria and speakers fees from AC Immune, Lilly, GE Healthcare, Janssen, USB, Schwabe, Esai, Pfizer, Novartis, and Roche. He has received a research grant paid to his institution from Schwabe. JP has received honoraria from Merz, Janssen-Cilag, and Novartis. MH has received a research grant from Schwabe GmbH, has received speakers honoraria from Pfizer Inc., Merz Pharmaceuticals, and GlaxoSmithKline, and served on an advisory board for Hoffmann-La Roche. ER is a Merz GmbH collaborator, is on the speakers bureau of/has received a travel grant from BMS, Lundbeck, Servier, and Otsouka, and has received a research grant from Lilly, BMS, AstraZeneca, and Lundbeck. FH has been a consultant to AstraZeneca in the area of depression between June 2011 and November 2012. WM has received payment for educational lectures from Merz. JW is on the advisory board for Eli Lilly and has received consulting fee or honorarium and support for traveling to board meetings. He received payment for lectures from Novartis. JK has received financial support for conducting clinical trials from various pharmaceutical companies manufacturing anti-dementia drugs. He is mentioned as coinventor on the following patents: Substituted piperidines or pyrrolidine compounds for treating sigma-receptor modulated disorders (WO001996031208A3); Method of differentially diagnosing dementias (WO002008058764A1); Soluble amyloid precursor proteins in CSF as biomarkers of Alzheimer’s disease (EP000002068151A1); Immunoglobulinbound Aβ and immunoglobulins-binding Aβ peptides in diagnosis and therapy of Alzheimer’s disease (WO002007082750A1); and Method of diagnosing acute cerebral ischemia (WO002008058764A1). The remaining authors declare that they have no competing interests.
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Winblad B, Palmer K, Kivipelto M, Jelic V, Fratiglioni L, Wahlund LO, et al. Mild cognitive impairment—beyond controversies, towards a consensus: report of the International Working Group on Mild Cognitive Impairment. J Intern Med. 2004;256:240–6. doi: 10.1111/j.1365-2796.2004.01380.x. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
