

Abdominal Aortic Calcifications Influences the Systemic and Renal Hemodynamic Response to Renal Denervation in the DENERHTN (Renal Denervation for Hypertension) Trial
- PMID: 29018027
- PMCID: PMC5721886
- DOI: 10.1161/JAHA.117.007062
Abdominal Aortic Calcifications Influences the Systemic and Renal Hemodynamic Response to Renal Denervation in the DENERHTN (Renal Denervation for Hypertension) Trial
Abstract
Background: The DENERHTN (Renal Denervation for Hypertension) trial confirmed the efficacy of renal denervation (RDN) in lowering daytime ambulatory systolic blood pressure when added to standardized stepped-care antihypertensive treatment (SSAHT) for resistant hypertension at 6 months.
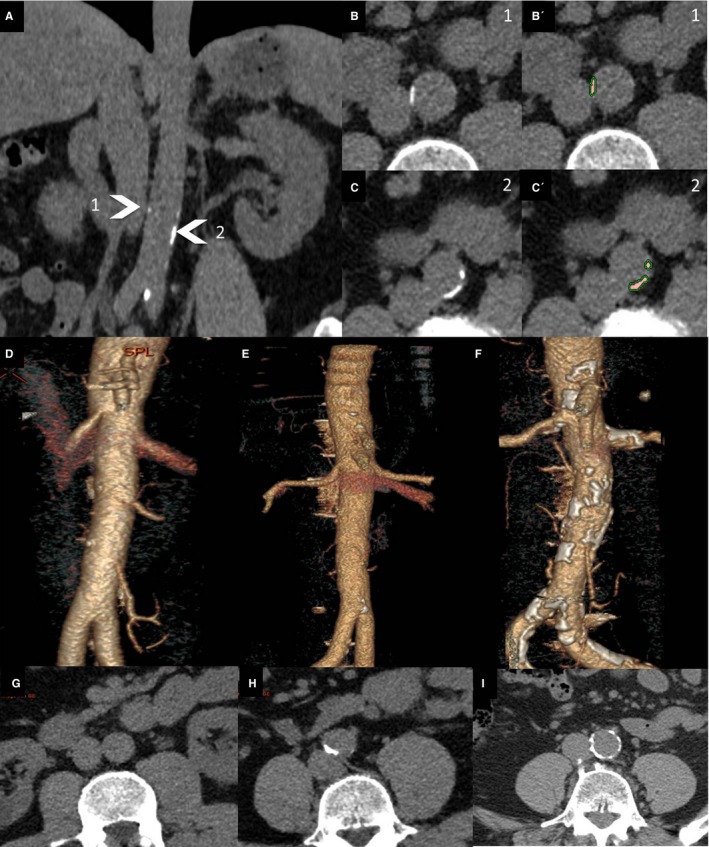
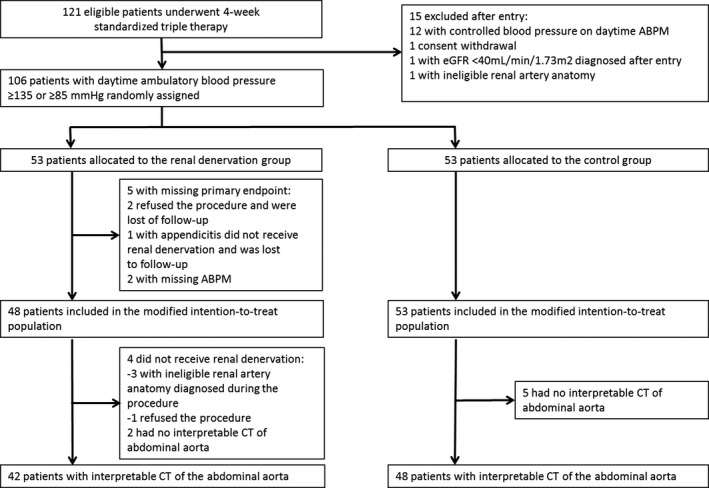
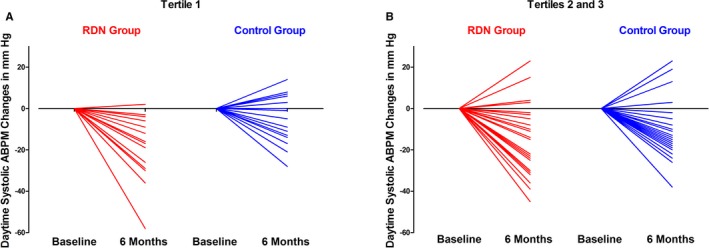
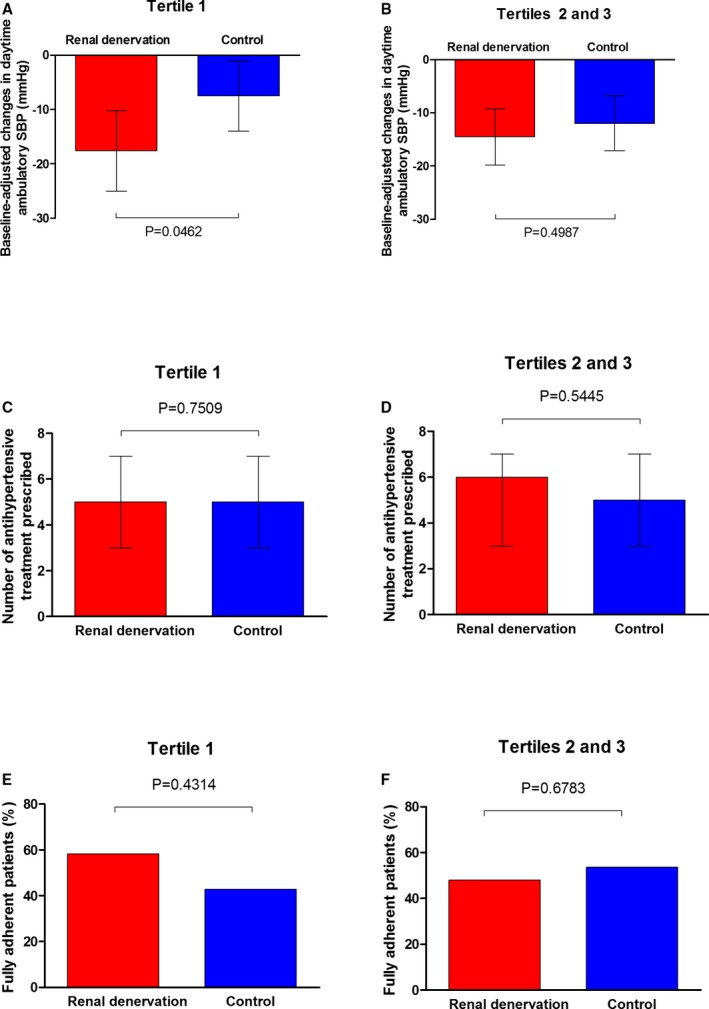
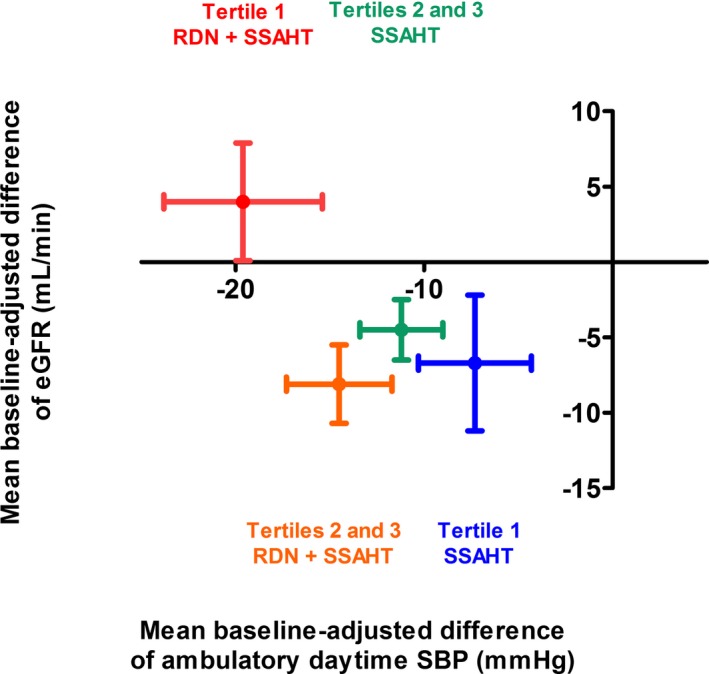
Methods and results: This post hoc exploratory analysis assessed the impact of abdominal aortic calcifications (AAC) on the hemodynamic and renal response to RDN at 6 months. In total, 106 patients with resistant hypertension were randomly assigned to RDN plus SSAHT or to the same SSAHT alone (control group). Total AAC volume was measured, with semiautomatic software and blind to randomization, from the aortic hiatus to the iliac bifurcation using the prerandomization noncontrast abdominal computed tomography scans of 90 patients. Measurements were expressed as tertiles. The baseline-adjusted difference in the change in daytime ambulatory systolic blood pressure from baseline to 6 months between the RDN and control groups was -10.1 mm Hg (P=0.0462) in the lowest tertile and -2.5 mm Hg (P=0.4987) in the 2 highest tertiles of AAC volume. Estimated glomerular filtration rate remained stable at 6 months for the patients in the lowest tertile of AAC volume who underwent RDN (+2.5 mL/min per 1.73 m2) but decreased in the control group (-8.0 mL/min per 1.73 m2, P=0.0148). In the 2 highest tertiles of AAC volume, estimated glomerular filtration rate decreased similarly in the RDN and control groups (P=0.2640).
Conclusions: RDN plus SSAHT resulted in a larger decrease in daytime ambulatory systolic blood pressure than SSAHT alone in patients with a lower AAC burden than in those with a higher AAC burden. This larger decrease in daytime ambulatory systolic blood pressure was not associated with a decrease in estimated glomerular filtration rate.
Clinical trial registration: URL: http://www.clinicaltrials.gov. Unique identifier: NCT01570777.
Keywords: antihypertensive therapy/sympathetic nervous system; aortic calcification; aortic disease; atherosclerosis; renal denervation; resistant hypertension.
© 2017 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
References
-
- Azizi M, Sapoval M, Gosse P, Monge M, Bobrie G, Delsart P, Midulla M, Mounier‐Vehier C, Courand PY, Lantelme P, Denolle T, Dourmap‐Collas C, Trillaud H, Pereira H, Plouin PF, Chatellier G. Optimum and stepped care standardised antihypertensive treatment with or without renal denervation for resistant hypertension (DENERHTN): a multicentre, open‐label, randomised controlled trial. Lancet. 2015;385:1957–1965. - PubMed
-
- Azizi M, Pereira H, Hamdidouche I, Gosse P, Monge M, Bobrie G, Delsart P, Mounier‐Vehier C, Courand PY, Lantelme P, Denolle T, Dourmap‐Collas C, Girerd X, Halimi JM, Zannad F, Ormezzano O, Vaisse B, Herpin D, Ribstein J, Chamontin B, Mourad JJ, Ferrari E, Plouin PF, Jullien V, Sapoval M, Chatellier G. Adherence to antihypertensive treatment and the blood pressure lowering effects of renal denervation in the renal denervation for hypertension (DENERHTN) trial. Circulation. 2016;134:847–857. - PubMed
-
- Gosse P, Cremer A, Pereira H, Bobrie G, Chatellier G, Chamontin B, Courand PY, Delsart P, Denolle T, Dourmap C, Ferrari E, Girerd X, Halimi JM, Herpin D, Lantelme P, Monge M, Mounier‐Vehier C, Mourad JJ, Ormezzano O, Ribstein J, Rossignol P, Sapoval M, Vaïsse B, Zannad F, Azizi M. Twenty‐four‐hour blood pressure monitoring to predict and assess impact of renal denervation: the DENERHTN Study (Renal Denervation for Hypertension). Hypertension. 2017;69:494–500. - PubMed
-
- Persu A, Kjeldsen S, Staessen JA, Azizi M. Renal denervation for treatment of hypertension: a second start and new challenges. Curr Hypertens Rep. 2016;18:6. - PubMed
-
- Mahfoud F, Böhm M, Azizi M, Pathak A, Durand Zaleski I, Ewen S, Tsioufis K, Andersson B, Blankestijn PJ, Burnier M, Chatellier G, Gafoor S, Grassi G, Joner M, Kjeldsen SE, Lüscher TF, Lobo MD, Lotan C, Parati G, Redon J, Ruilope L, Sudano I, Ukena C, van Leeuwen E, Volpe M, Windecker S, Witkowski A, Wijns W, Zeller T, Schmieder RE. Proceedings from the European clinical consensus conference for renal denervation: considerations on future clinical trial design. Eur Heart J. 2015;36:2219–2227. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
