

Post-abortion care with misoprostol - equally effective, safe and accepted when administered by midwives compared to physicians: a randomised controlled equivalence trial in a low-resource setting in Kenya
- PMID: 29018067
- PMCID: PMC5652492
- DOI: 10.1136/bmjopen-2017-016157
Post-abortion care with misoprostol - equally effective, safe and accepted when administered by midwives compared to physicians: a randomised controlled equivalence trial in a low-resource setting in Kenya
Abstract
Objective: To assess the effectiveness of midwives administering misoprostol to women with incomplete abortion seeking post-abortion care (PAC), compared with physicians.
Design: A multicentre randomised controlled equivalence trial. The study was not masked.
Settings: Gynaecological departments in two hospitals in a low-resource setting, Kenya.
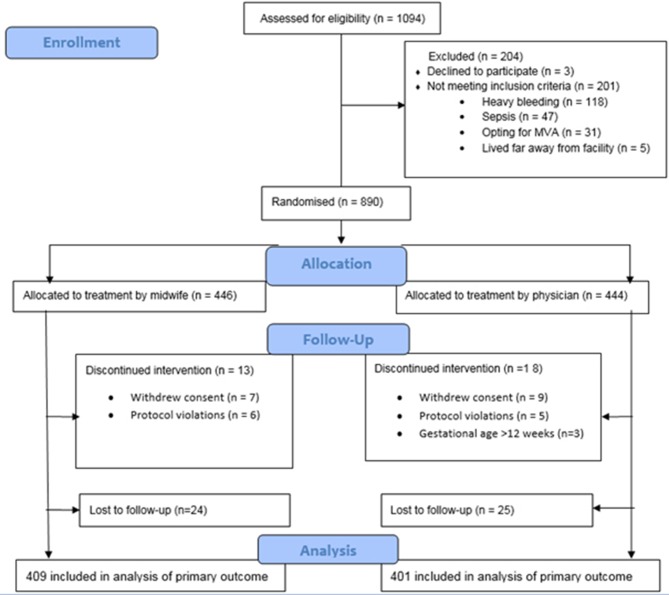
Population: Women (n=1094) with incomplete abortion in the first trimester, seeking PAC between 1 June 2013 to 31 May 2016. Participants were randomly assigned to receive treatment from midwives or physicians. 409 and 401 women in the midwife and physician groups, respectively, were included in the per-protocol analysis.
Interventions: 600 µg misoprostol orally, and contraceptive counselling by a physician or midwife.
Main outcome measures: Complete abortion not needing surgical intervention within 7-10 days. The main outcome was analysed on the per-protocol population with a generalised estimating equation model. The predefined equivalence range was -4% to 4%. Secondary outcomes were analysed descriptively.
Results: The proportion of complete abortion was 94.8% (768/810): 390 (95.4%) in the midwife group and 378 (94.3%) in the physician group. The proportion of incomplete abortion was 5.2% (42/810), similarly distributed between midwives and physicians. The model-based risk difference for midwives versus physicians was 1.0% (-4.1 to 2.2). Most women felt safe (97%; 779/799), and 93% (748/801) perceived the treatment as expected/easier than expected. After contraceptive counselling the uptake of a contraceptive method after 7-10 days occurred in 76% (613/810). No serious adverse events were recorded.
Conclusions: Treatment of incomplete abortion with misoprostol provided by midwives is equally effective, safe and accepted by women as when administered by physicians in a low-resource setting. Systematically provided contraceptive counselling in PAC is effective to mitigate unmet need for contraception.
Trial registration number: NCT01865136; Results.
Keywords: Community Gynaecology; Health Policy; Maternal Medicine; Reproductive Medicine.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2017. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
References
-
- Safe abortion: technical and policy guidance for health systems, second edition 12. Geneva: World Health Organization, 2012. http://apps.who.int/iris/bitstream/10665/70914/1/9789241548434_eng.pdf (accessed 20 Jul 2017). - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical