

Randomized Crossover Trial of Blood Volume Monitoring-Guided Ultrafiltration Biofeedback to Reduce Intradialytic Hypotensive Episodes with Hemodialysis
- PMID: 29018100
- PMCID: PMC5672962
- DOI: 10.2215/CJN.01030117
Randomized Crossover Trial of Blood Volume Monitoring-Guided Ultrafiltration Biofeedback to Reduce Intradialytic Hypotensive Episodes with Hemodialysis
Abstract
Background and objectives: Intradialytic hypotension (IDH) is associated with morbidity. The effect of blood volume-guided ultrafiltration biofeedback, which automatically adjusts fluid removal rate on the basis of blood volume parameters, on the reduction of IDH was tested in a randomized crossover trial.
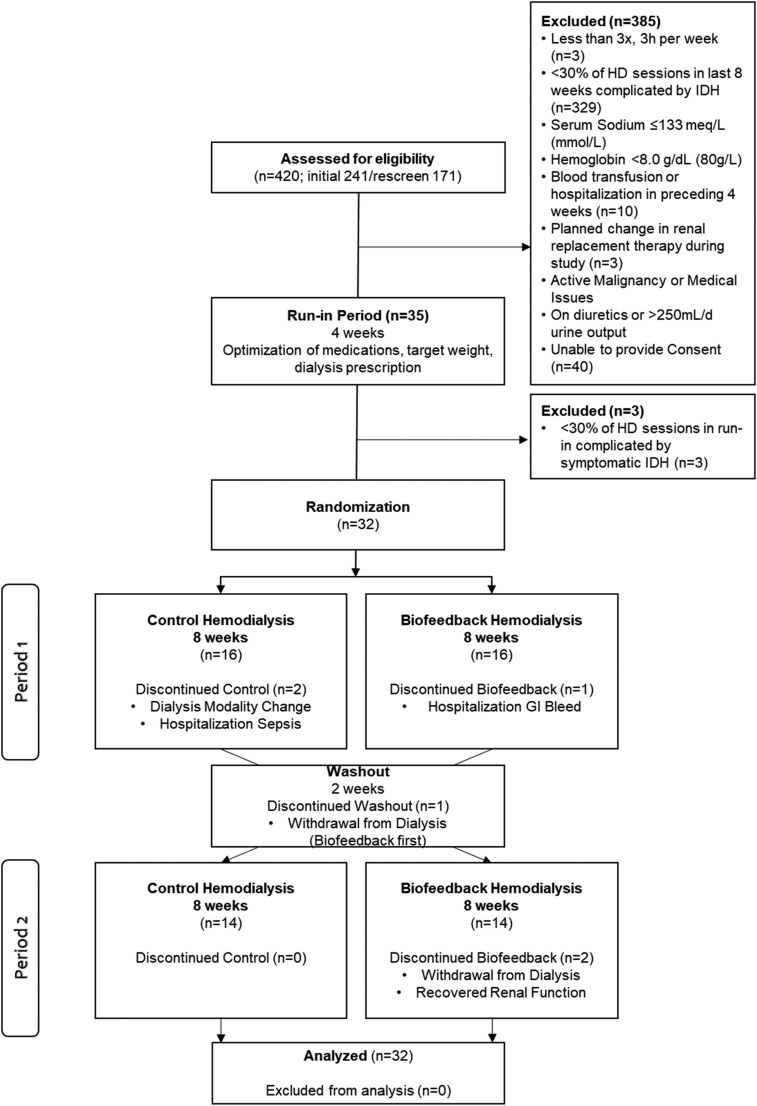
Design, setting, participants, & measurements: We performed a 22-week, single blind, randomized crossover trial in patients receiving maintenance hemodialysis who had >30% of sessions complicated by symptomatic IDH in five centers in Calgary, Alberta, Canada. Participants underwent a 4-week run-in period to standardize dialysis prescription and dry weight on the basis of clinical examination. Those meeting inclusion criteria were randomized to best clinical practice hemodialysis (control) or best clinical practice plus blood volume-guided ultrafiltration biofeedback (intervention) for 8 weeks, followed by a 2-week washout and subsequent crossover for a second 8-week phase. The primary outcome was rate of symptomatic IDH.
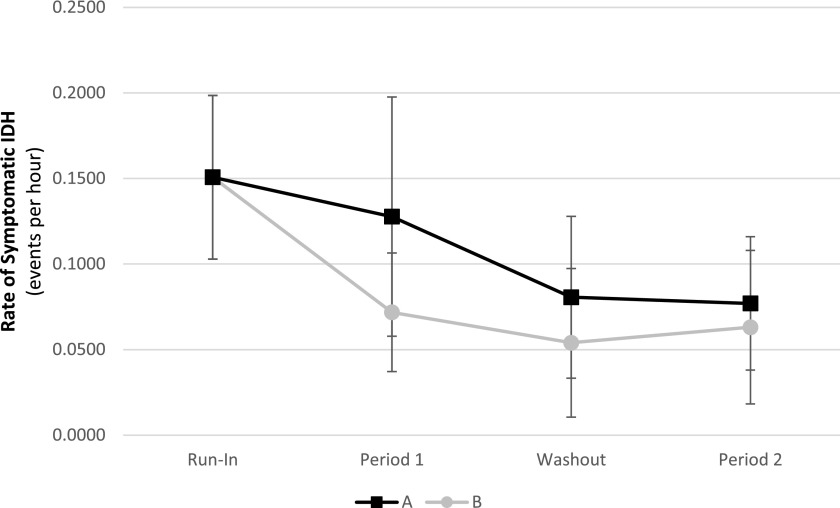
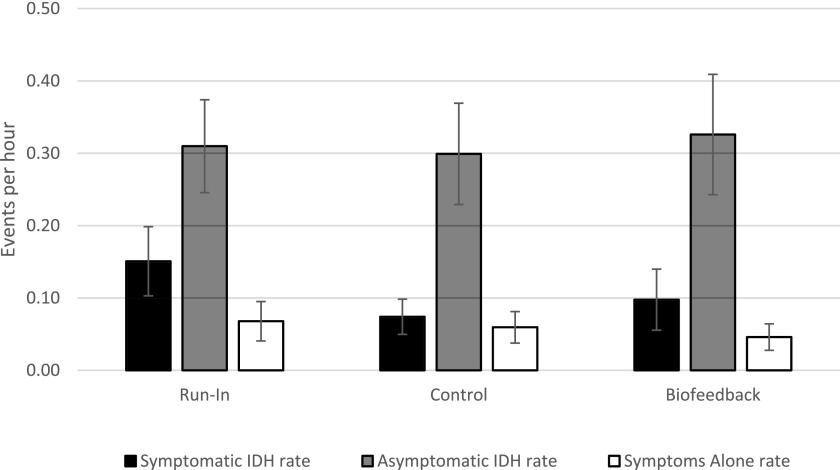
Results: Thirty-five participants entered, 32 were randomized, and 26 completed the study. The rate of symptomatic IDH with biofeedback was 0.10/h (95% confidence interval, 0.06 to 0.14) and 0.07/h (95% confidence interval, 0.05 to 0.10) during control (P=0.29). There were no differences in the rate or proportion of sessions with asymptomatic IDH or symptoms alone. Results remained consistent when adjusted for randomization order and study week. There were no differences between intervention and control in the last study week in interdialytic weight gain (difference [SD], -0.02 [0.8] kg), brain natriuretic peptide (1460 [19,052] ng/L), cardiac troponins (3 [86] ng/L), extracellular water-to-intracellular water ratio (0.05 [0.33]), ultrafiltration rate (1.1 [7.0] ml/kg per hour), and dialysis recovery time (0.43 [19.25] hours).
Conclusion: The use of blood volume monitoring-guided ultrafiltration biofeedback in patients prone to IDH did not reduce the rate of symptomatic IDH events.
Keywords: Alberta; Biofeedback, Psychology; Blood Volume; Canada; Confidence Intervals; Cross-Over Studies; Fluid Therapy; Natriuretic Peptide, Brain; Random Allocation; Single-Blind Method; Troponin; Water; Weight Gain; biofeedback; hemodialysis; hypotension; intradialytic hypotension; randomized controlled trials; renal dialysis; ultrafiltration.
Copyright © 2017 by the American Society of Nephrology.
Figures

Comment in
-
Feedback Control in Hemodialysis-Much Ado about Nothing?Clin J Am Soc Nephrol. 2017 Nov 7;12(11):1730-1732. doi: 10.2215/CJN.09770917. Epub 2017 Oct 10. Clin J Am Soc Nephrol. 2017. PMID: 29018099 Free PMC article. No abstract available.
Similar articles
-
Ultrafiltration biofeedback guided by blood volume monitoring to reduce intradialytic hypotensive episodes in hemodialysis: study protocol for a randomized controlled trial.Trials. 2014 Dec 10;15:483. doi: 10.1186/1745-6215-15-483. Trials. 2014. PMID: 25496294 Free PMC article. Clinical Trial.
-
[Effect of automated blood volume control on the incidence of intra-dialysis hypotension].Acta Med Croatica. 2003;57(1):17-22. Acta Med Croatica. 2003. PMID: 12876857 Croatian.
-
Efficacy of hemocontrol biofeedback system in intradialytic hypotension-prone hemodialysis patients.J Korean Med Sci. 2014 Jun;29(6):805-10. doi: 10.3346/jkms.2014.29.6.805. Epub 2014 May 30. J Korean Med Sci. 2014. PMID: 24932082 Free PMC article.
-
How can we prevent intradialytic hypotension?Curr Opin Nephrol Hypertens. 2012 Nov;21(6):593-9. doi: 10.1097/MNH.0b013e3283588f3c. Curr Opin Nephrol Hypertens. 2012. PMID: 22914686 Review.
-
Intensive Hemodialysis and Treatment Complications and Tolerability.Am J Kidney Dis. 2016 Nov;68(5S1):S43-S50. doi: 10.1053/j.ajkd.2016.05.021. Am J Kidney Dis. 2016. PMID: 27772642 Review.
Cited by
-
Assessing accuracy of estimated dry weight in dialysis patients post transplantation: the kidney knows best.J Nephrol. 2021 Dec;34(6):2093-2097. doi: 10.1007/s40620-021-01029-7. Epub 2021 May 24. J Nephrol. 2021. PMID: 34031847 Free PMC article.
-
How to Limit Interdialytic Weight Gain in Patients on Maintenance Hemodialysis: State of the Art and Perspectives.J Clin Med. 2025 Mar 9;14(6):1846. doi: 10.3390/jcm14061846. J Clin Med. 2025. PMID: 40142654 Free PMC article. Review.
-
Feedback control in hemodialysis.Semin Dial. 2025 Jan-Feb;38(1):62-70. doi: 10.1111/sdi.13185. Epub 2023 Nov 23. Semin Dial. 2025. PMID: 37994191 Free PMC article. Review.
-
Progress in volume assessment for the hemodialysis patients.Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2021 Jul 28;46(7):759-766. doi: 10.11817/j.issn.1672-7347.2021.200783. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2021. PMID: 34382594 Free PMC article. Chinese, English.
-
Individualization of Ultrafiltration in Hemodialysis.IEEE Trans Biomed Eng. 2019 Aug;66(8):2174-2181. doi: 10.1109/TBME.2018.2884931. Epub 2018 Dec 4. IEEE Trans Biomed Eng. 2019. PMID: 30530307 Free PMC article.
References
-
- Zager PG, Nikolic J, Brown RH, Campbell MA, Hunt WC, Peterson D, Van Stone J, Levey A, Meyer KB, Klag MJ, Johnson HK, Clark E, Sadler JH, Teredesai P: “U” curve association of blood pressure and mortality in hemodialysis patients. Medical Directors of Dialysis Clinic, Inc. Kidney Int 54: 561–569, 1998 - PubMed
-
- Shoji T, Tsubakihara Y, Fujii M, Imai E: Hemodialysis-associated hypotension as an independent risk factor for two-year mortality in hemodialysis patients. Kidney Int 66: 1212–1220, 2004 - PubMed
-
- Yoshimitsu T, Hirakata H, Fujii K, Kanai H, Hirakata E, Higashi H, Kubo M, Tanaka H, Shinozaki M, Katafuchi R, Yokomizo Y, Oh Y, Tomooka S, Fujimi S, Fujishima M: Cerebral ischemia as a causative mechanism for rapid progression of brain atrophy in chronic hemodialysis patients. Clin Nephrol 53: 445–451, 2000 - PubMed
-
- Ishida I, Hirakata H, Sugimori H, Omae T, Hirakata E, Ibayashi S, Kubo M, Fujishima M: Hemodialysis causes severe orthostatic reduction in cerebral blood flow velocity in diabetic patients. Am J Kidney Dis 34: 1096–1104, 1999 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
