

Preferential Impairment of the Contralesional Posterior Semicircular Canal in Internuclear Ophthalmoplegia
- PMID: 29018402
- PMCID: PMC5614936
- DOI: 10.3389/fneur.2017.00502
Preferential Impairment of the Contralesional Posterior Semicircular Canal in Internuclear Ophthalmoplegia
Abstract
Background: The vertical vestibulo-ocular reflex (VOR) may be impaired in internuclear ophthalmoplegia (INO) as the medial longitudinal fasciculus (MLF) conveys VOR-signals from the vertical semicircular canals. It has been proposed that signals from the contralesional posterior semicircular canal (PSC) are exclusively transmitted through the MLF, while for the contralesional anterior canal other pathways exist.
Objective: Here, we aimed to characterize dysfunction in individual canals in INO-patients using the video-head-impulse test (vHIT) and to test the hypothesis of dissociated vertical canal impairment in INO.
Methods: Video-head-impulse testing and magnetic resonance imaging were obtained in 21 consecutive patients with unilateral (n = 16) or bilateral (n = 5) INO and 42 controls. VOR-gains and compensatory catch-up saccades were analyzed and the overall function (normal vs. impaired) of each semicircular canal was rated.
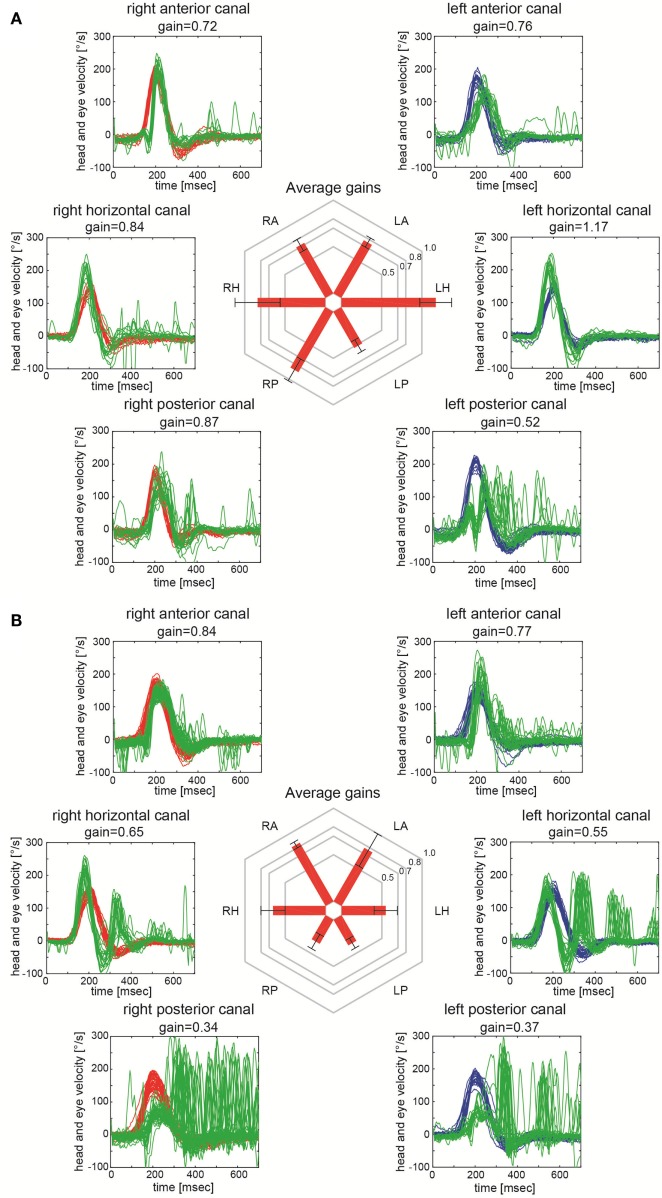
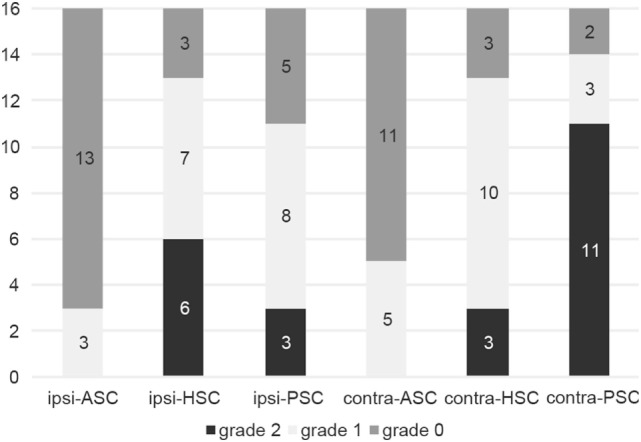
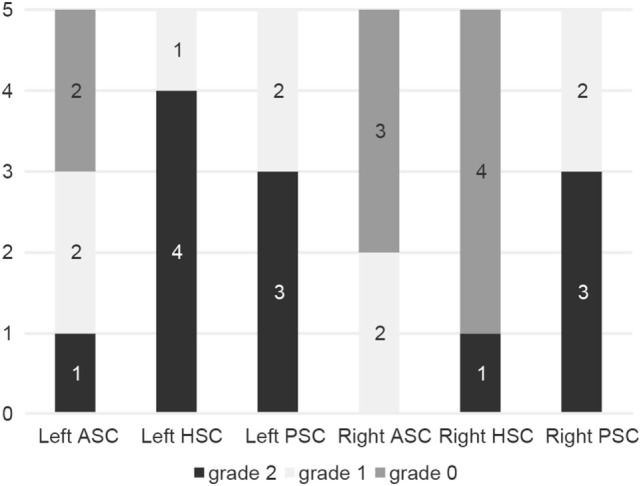
Results: In unilateral INO, largest VOR-gain reductions were noted in the contralesional PSC (0.55 ± 0.11 vs. 0.89 ± 0.08, p < 0.001), while in bilateral INO both posterior (0.43 ± 0.11 vs. 0.89 ± 0.08, p < 0.001) and anterior (0.58 ± 0.19 vs. 0.88 ± 0.09, p < 0.001) canals showed marked drops. Small, but significant VOR-gain reductions were also found in the other canals in unilateral and bilateral INO-patients. Impairment of overall canal function was restricted to the contralesional posterior canal in 60% of unilateral INO-patients, while isolated involvement of the posterior canal was rare in bilateral INO-patients (20%). Reviewers correctly identified the INO-pattern in 15/21 (71%) patients and in all controls (sensitivity = 84.2% [95%-CI = 0.59.5-95.8]; specificity = 95.5% [95%-CI = 83.3-99.2]).
Conclusion: Using a vHIT based overall rating of canal function, the correct INO-pattern could be identified with high accuracy. The predominant and often selective impairment of the contralesional posterior canal in unilateral INO further supports the role of the MLF in transmitting posterior canal signals. In patients with acute dizziness and abnormal vHIT-results, central pathologies such as INO should be considered as well, especially when the posterior canal is involved.
Keywords: compensatory saccade; head impulse test; internuclear ophthalmoplegia; medial longitudinal fasciculus; vestibulo-ocular reflex.
Figures
Similar articles
-
Vestibulo-ocular reflex deficits with medial longitudinal fasciculus lesions.J Neurol. 2017 Oct;264(10):2119-2129. doi: 10.1007/s00415-017-8607-8. Epub 2017 Sep 6. J Neurol. 2017. PMID: 28879396
-
Mild Bilateral Internuclear Ophthalmoplegia: The Diagnostic Role of the Vertical Posterior Canal Vestibulo-Ocular Reflex in Acute Brainstem Demyelination, a Clinical-Radiologic Correlation.J Neuroophthalmol. 2022 Mar 1;42(1):e281-e288. doi: 10.1097/WNO.0000000000001262. Epub 2021 Apr 26. J Neuroophthalmol. 2022. PMID: 34001732
-
Vestibulo-Ocular Reflex Abnormalities in Posterior Semicircular Canal Benign Paroxysmal Positional Vertigo: A Pilot Study.Iran J Otorhinolaryngol. 2017 Sep;29(94):269-274. Iran J Otorhinolaryngol. 2017. PMID: 28955674 Free PMC article.
-
Video head impulse test: a review of the literature.Eur Arch Otorhinolaryngol. 2017 Mar;274(3):1215-1222. doi: 10.1007/s00405-016-4157-4. Epub 2016 Jun 21. Eur Arch Otorhinolaryngol. 2017. PMID: 27328962 Review.
-
VOR gain of lateral semicircular canal using video head impulse test in acute unilateral vestibular hypofunction: A systematic review.Front Neurol. 2022 Dec 8;13:948462. doi: 10.3389/fneur.2022.948462. eCollection 2022. Front Neurol. 2022. PMID: 36570452 Free PMC article.
Cited by
-
Unique compensatory oculomotor behavior in people living with multiple sclerosis.J Neurol Sci. 2022 Nov 15;442:120411. doi: 10.1016/j.jns.2022.120411. Epub 2022 Sep 6. J Neurol Sci. 2022. PMID: 36088792 Free PMC article.
-
Vascular vertigo: updates.J Neurol. 2019 Aug;266(8):1835-1843. doi: 10.1007/s00415-018-9040-3. Epub 2018 Sep 5. J Neurol. 2019. PMID: 30187161 Review.
-
Eye Movement Abnormalities in Multiple Sclerosis: Pathogenesis, Modeling, and Treatment.Front Neurol. 2018 Feb 5;9:31. doi: 10.3389/fneur.2018.00031. eCollection 2018. Front Neurol. 2018. PMID: 29467711 Free PMC article. Review.
-
Greater Disability Is Associated with Worse Vestibular and Compensatory Oculomotor Functions in People Living with Multiple Sclerosis.Brain Sci. 2022 Nov 9;12(11):1519. doi: 10.3390/brainsci12111519. Brain Sci. 2022. PMID: 36358444 Free PMC article.
-
Case report: A disconjugate pattern in video head impulse testing hints toward a central cause of acute vertigo.Front Neurol. 2023 Jul 27;14:1222475. doi: 10.3389/fneur.2023.1222475. eCollection 2023. Front Neurol. 2023. PMID: 37576019 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources