

Socioeconomic Outcome and Quality of Life in Adults after Status Epilepticus: A Multicenter, Longitudinal, Matched Case-Control Analysis from Germany
- PMID: 29018404
- PMCID: PMC5622933
- DOI: 10.3389/fneur.2017.00507
Socioeconomic Outcome and Quality of Life in Adults after Status Epilepticus: A Multicenter, Longitudinal, Matched Case-Control Analysis from Germany
Abstract
Background: There is a lack of data concerning socioeconomic outcome and quality of life (QoL) in patients after status epilepticus (SE) in Germany.
Patients and methods: Adult patients treated between 2011 and 2015 due to SE at the university hospitals in Frankfurt, Greifswald, and Marburg were asked to fill out a questionnaire regarding long-term outcome of at least 3 months after discharge. The SE cohort consisted of 25.9% patients with an acute symptomatic, 42% with a remote symptomatic and previous epilepsy, 22.2% with a new-onset remote symptomatic, and 9.9% with other or unknown etiology. A matched case-control analysis was applied for comparison with patients with drug refractory epilepsy and seizure remission, both not previously affected by SE.
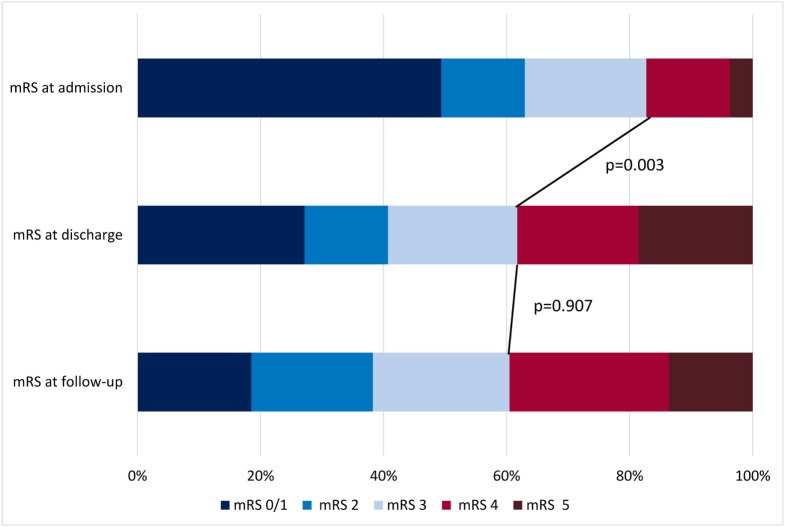
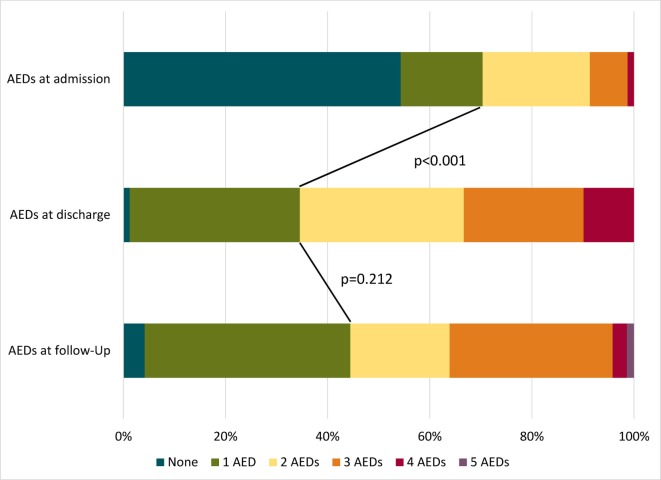
Results: A total of 81 patients (mean age: 58.7 ± 18.0 years; 58% female) participated. A non-refractory course was present in 59.3%, while 27.2% had a refractory SE (RSE) and 13.6% had a superrefractory SE (SRSE). Before admission, a favorable modified Rankin Scale (mRS) of 0-3 was found in 82.7% (67/81), deteriorating to 38.3% (31/81) (p = 0.003) at discharge. The majority returned home [51.9% (42/81)], 32.1% entered a rehabilitation facility, while 12.3% were transferred to a nursing home and 3.7% to another hospital. The overall mRS at follow-up did not change; 61.8% (45/74) reached an mRS of 0-3. In RSE and SRSE, the proportion with a favorable mRS increased from 45.5% at discharge to 70% at follow-up, while QoL was comparable to a non-refractory SE course. Matched epilepsy controls in seizure remission were treated with a lower mean number of anticonvulsants (1.3 ± 0.7) compared to controls with drug refractory epilepsy (1.9 ± 0.8; p < 0.001) or SE (1.9 ± 1.1; p < 0.001). A major depression was found in 32.8% of patients with SE and in 36.8% of drug refractory epilepsy, but only in 20.3% of patients in seizure remission. QoL was reduced in all categories (QOLIE-31) in SE patients in comparison with patients in seizure remission, but was comparable to patients with drug refractory epilepsy.
Discussion: Patients after SE show substantial impairments in their QoL and daily life activities. However, in the long term, patients with RSE and SRSE had a relatively favorable outcome comparable to that of patients with a non-refractory SE course. This underlines the need for efficient therapeutic options in SE.
Keywords: anticonvulsants; epilepsy; morbidity; mortality; seizure.
Figures
Similar articles
-
Long-term outcome of refractory status epilepticus in adults: A retrospective population-based study.Epilepsy Res. 2017 Jul;133:13-21. doi: 10.1016/j.eplepsyres.2017.03.009. Epub 2017 Apr 2. Epilepsy Res. 2017. PMID: 28402834
-
Outcome of emergency neurosurgery in patients with refractory and super-refractory status epilepticus: a systematic review and individual participant data meta-analysis.Front Neurol. 2024 May 28;15:1403266. doi: 10.3389/fneur.2024.1403266. eCollection 2024. Front Neurol. 2024. PMID: 38863514 Free PMC article.
-
Costs and cost-driving factors for acute treatment of adults with status epilepticus: A multicenter cohort study from Germany.Epilepsia. 2016 Dec;57(12):2056-2066. doi: 10.1111/epi.13584. Epub 2016 Oct 18. Epilepsia. 2016. PMID: 27753082
-
Factors associated with occurrence and outcome of super-refractory status epilepticus.Seizure. 2017 Nov;52:53-59. doi: 10.1016/j.seizure.2017.09.003. Epub 2017 Sep 9. Seizure. 2017. PMID: 28963934
-
Efficacy and safety of perampanel in refractory and super-refractory status epilepticus: cohort study of 81 patients and literature review.J Neurol. 2021 Oct;268(10):3744-3757. doi: 10.1007/s00415-021-10506-9. Epub 2021 Mar 22. J Neurol. 2021. PMID: 33754209 Review.
Cited by
-
Opportunities for and Challenges of Pulmonary Drug Delivery in the Management of Acute Exacerbations of CNS Disorders.CNS Drugs. 2025 Aug 7. doi: 10.1007/s40263-025-01213-4. Online ahead of print. CNS Drugs. 2025. PMID: 40775197 Review.
-
Status epilepticus in patients with brain tumors and metastases: A multicenter cohort study of 208 patients and literature review.Neurol Res Pract. 2024 Apr 4;6(1):19. doi: 10.1186/s42466-024-00314-7. Neurol Res Pract. 2024. PMID: 38570823 Free PMC article.
-
[Acceptance, demand, reasons for consultation and outcome of counseling on epilepsy in Hesse and Lower Franconia].Nervenarzt. 2019 Aug;90(8):832-839. doi: 10.1007/s00115-019-0676-8. Nervenarzt. 2019. PMID: 30694366 German.
-
Acute-on-chronic subdural hematoma: a new entity for prophylactic anti-epileptic treatment?Eur J Trauma Emerg Surg. 2022 Apr;48(2):933-942. doi: 10.1007/s00068-020-01508-9. Epub 2020 Sep 28. Eur J Trauma Emerg Surg. 2022. PMID: 32986132 Free PMC article.
-
[S2k guidelines: status epilepticus in adulthood : Guidelines of the German Society for Neurology].Nervenarzt. 2021 Oct;92(10):1002-1030. doi: 10.1007/s00115-020-01036-2. Epub 2021 Mar 22. Nervenarzt. 2021. PMID: 33751150 Free PMC article. Review. German.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources