

The continuous reaction time test for minimal hepatic encephalopathy validated by a randomized controlled multi-modal intervention-A pilot study
- PMID: 29020023
- PMCID: PMC5636096
- DOI: 10.1371/journal.pone.0185412
The continuous reaction time test for minimal hepatic encephalopathy validated by a randomized controlled multi-modal intervention-A pilot study
Abstract
Background: Minimal hepatic encephalopathy (MHE) is clinically undetectable and the diagnosis requires psychometric tests. However, a lack of clarity exists as to whether the tests are in fact able to detect changes in cognition.
Aim: To examine if the continuous reaction time test (CRT) can detect changes in cognition with anti-HE intervention in patients with cirrhosis and without clinically manifest hepatic encephalopathy (HE).
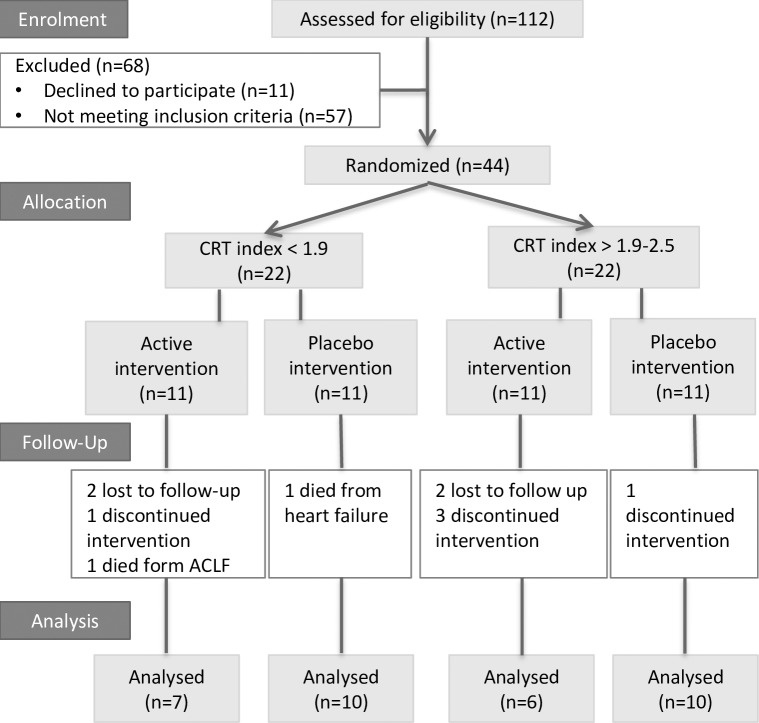
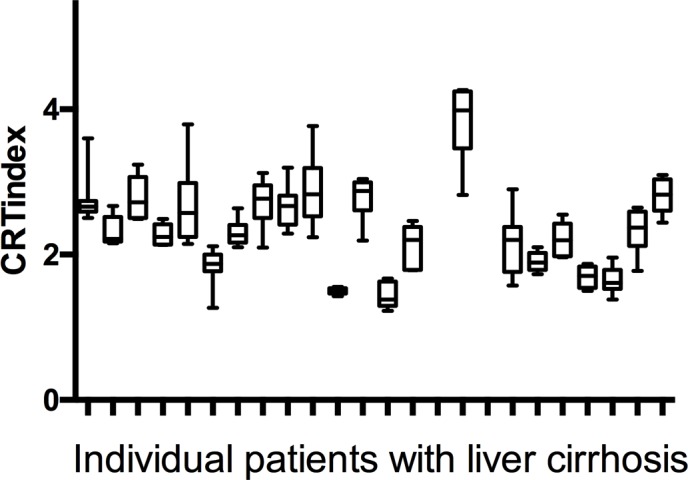
Methods: Firstly, we conducted a reproducibility analysis and secondly measured change in CRT induced by anti-HE treatment in a randomized controlled pilot study: We stratified 44 patients with liver cirrhosis and without clinically manifest HE according to a normal (n = 22) or abnormal (n = 22) CRT. Each stratum was then block randomized to receive multimodal anti-HE intervention (lactulose+branched-chain amino acids+rifaximin) or triple placebos for 3 months in a double-blinded fashion. The CRT is a simple PC-based test and the test result, the CRT index (normal threshold > 1.9), describes the patient's stability of alertness during the 10-minute test. Our study outcome was the change in CRT index in each group at study exit. The portosystemic encephalopathy (PSE) test, a paper-and-pencil test battery (normal threshold above -5), was used as a comparator test according to international guidelines.
Results: The patients with an abnormal CRT index who were randomized to receive the active intervention normalized or improved their CRT index (mean change 0.92 ± 0.29, p = 0.01). Additionally, their PSE improved (change 3.85 ± 1.83, p = 0.03). There was no such effect in any of the other study groups.
Conclusion: In this cohort of patients with liver cirrhosis and no manifest HE, the CRT identified a group in whom cognition improved with intensive anti-HE intervention. This finding infers that the CRT can detect a response to treatment and might help in selecting patients for treatment.
Conflict of interest statement
Figures
References
-
- Maldonado-Garza HJ, Vazquez-Elizondo G, Gaytan-Torres JO, Flores-Rendon AR, Cardenas-Sandoval MG, Bosques-Padilla FJ. Prevalence of minimal hepatic encephalopathy in cirrhotic patients. Ann Hepatol. 2011;10 Suppl 2:S40–4. Epub 2012/01/18. doi: 951128 [pii]. . - PubMed
-
- Li YY, Nie YQ, Sha WH, Zeng Z, Yang FY, Ping L, et al. Prevalence of subclinical hepatic encephalopathy in cirrhotic patients in China. World J Gastroenterol. 2004;10(16):2397–401. Epub 2004/07/31. doi: 10.3748/wjg.v10.i16.2397 . - DOI - PMC - PubMed
-
- Gluud LL, Vilstrup H, Morgan MY. The effect of treatment for hepatic encephalopathy with nonabsorbable disaccarides on morbidity and mortality in patients with cirrhosis: Systematic review and meta-analysis In: Jalan R, editor. EASL International Liver Congress 2015; Vienna: ILC 2015 Absctract Book: EASL; 2015. p. 175.
-
- Lauridsen MM, Bajaj JS. Hepatic Encephalopathy Treatment and Driving: A Continental Divide. J Hepatol. 2015. doi: 10.1016/j.jhep.2015.03.017 . - DOI - PubMed
-
- Weissenborn K. Psychometric tests for diagnosing minimal hepatic encephalopathy. Metab Brain Dis. 2012. Epub 2012/09/21. doi: 10.1007/s11011-012-9336-4 . - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
