

Data-Adaptive Estimation for Double-Robust Methods in Population-Based Cancer Epidemiology: Risk Differences for Lung Cancer Mortality by Emergency Presentation
- PMID: 29020131
- PMCID: PMC5888939
- DOI: 10.1093/aje/kwx317
Data-Adaptive Estimation for Double-Robust Methods in Population-Based Cancer Epidemiology: Risk Differences for Lung Cancer Mortality by Emergency Presentation
Abstract
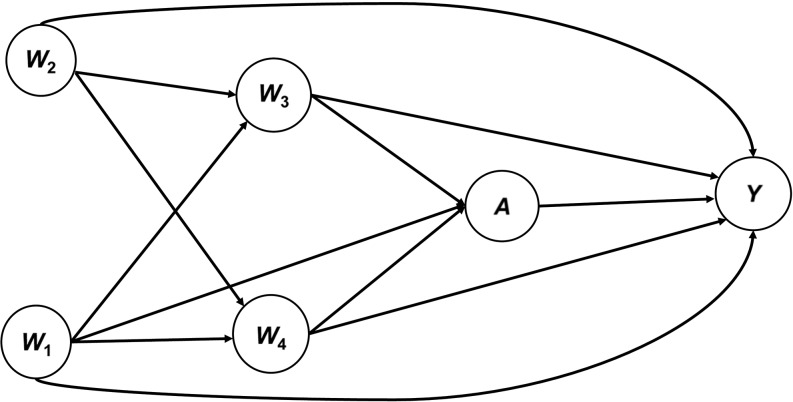
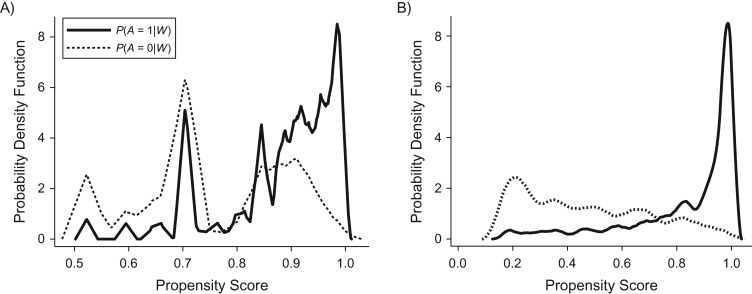
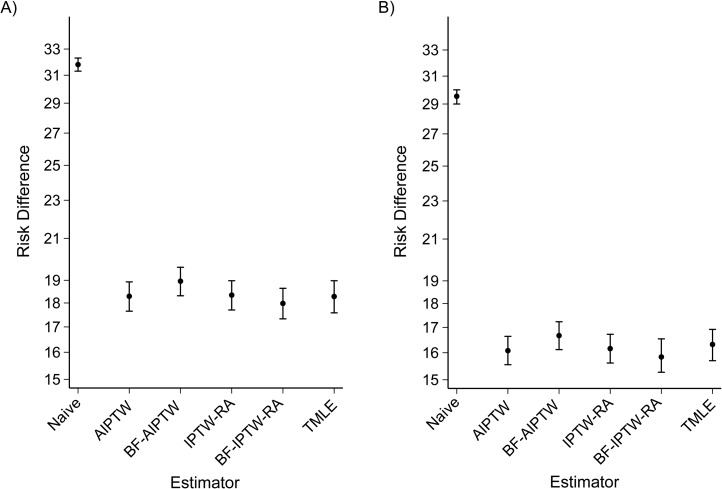
In this paper, we propose a structural framework for population-based cancer epidemiology and evaluate the performance of double-robust estimators for a binary exposure in cancer mortality. We conduct numerical analyses to study the bias and efficiency of these estimators. Furthermore, we compare 2 different model selection strategies based on 1) Akaike's Information Criterion and the Bayesian Information Criterion and 2) machine learning algorithms, and we illustrate double-robust estimators' performance in a real-world setting. In simulations with correctly specified models and near-positivity violations, all but the naive estimators had relatively good performance. However, the augmented inverse-probability-of-treatment weighting estimator showed the largest relative bias. Under dual model misspecification and near-positivity violations, all double-robust estimators were biased. Nevertheless, the targeted maximum likelihood estimator showed the best bias-variance trade-off, more precise estimates, and appropriate 95% confidence interval coverage, supporting the use of the data-adaptive model selection strategies based on machine learning algorithms. We applied these methods to estimate adjusted 1-year mortality risk differences in 183,426 lung cancer patients diagnosed after admittance to an emergency department versus persons with a nonemergency cancer diagnosis in England (2006-2013). The adjusted mortality risk (for patients diagnosed with lung cancer after admittance to an emergency department) was 16% higher in men and 18% higher in women, suggesting the importance of interventions targeting early detection of lung cancer signs and symptoms.
Figures
Similar articles
-
Double Robust Efficient Estimators of Longitudinal Treatment Effects: Comparative Performance in Simulations and a Case Study.Int J Biostat. 2019 Feb 26;15(2):/j/ijb.2019.15.issue-2/ijb-2017-0054/ijb-2017-0054.xml. doi: 10.1515/ijb-2017-0054. Int J Biostat. 2019. PMID: 30811344 Free PMC article.
-
Effect Estimation in Point-Exposure Studies with Binary Outcomes and High-Dimensional Covariate Data - A Comparison of Targeted Maximum Likelihood Estimation and Inverse Probability of Treatment Weighting.Int J Biostat. 2016 Nov 1;12(2):/j/ijb.2016.12.issue-2/ijb-2015-0034/ijb-2015-0034.xml. doi: 10.1515/ijb-2015-0034. Int J Biostat. 2016. PMID: 27889705 Free PMC article.
-
Collaborative double robust targeted maximum likelihood estimation.Int J Biostat. 2010 May 17;6(1):Article 17. doi: 10.2202/1557-4679.1181. Int J Biostat. 2010. PMID: 20628637 Free PMC article.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Interval estimation of risk ratio in the simple compliance randomized trial.Contemp Clin Trials. 2007 Feb;28(2):120-9. doi: 10.1016/j.cct.2006.05.005. Epub 2006 Jul 3. Contemp Clin Trials. 2007. PMID: 16820329 Review.
Cited by
-
Comparison of Parametric and Nonparametric Estimators for the Association Between Incident Prepregnancy Obesity and Stillbirth in a Population-Based Cohort Study.Am J Epidemiol. 2019 Jul 1;188(7):1328-1336. doi: 10.1093/aje/kwz081. Am J Epidemiol. 2019. PMID: 31111944 Free PMC article.
-
Stacked generalization: an introduction to super learning.Eur J Epidemiol. 2018 May;33(5):459-464. doi: 10.1007/s10654-018-0390-z. Epub 2018 Apr 10. Eur J Epidemiol. 2018. PMID: 29637384 Free PMC article. Review.
-
Deep Ensemble Machine Learning Framework for the Estimation of Concentrations.Environ Health Perspect. 2022 Mar;130(3):37004. doi: 10.1289/EHP9752. Epub 2022 Mar 7. Environ Health Perspect. 2022. PMID: 35254864 Free PMC article.
-
Association of medical male circumcision and sexually transmitted infections in a population-based study using targeted maximum likelihood estimation.BMC Public Health. 2021 Sep 8;21(1):1642. doi: 10.1186/s12889-021-11705-9. BMC Public Health. 2021. PMID: 34496810 Free PMC article.
-
Using longitudinal targeted maximum likelihood estimation in complex settings with dynamic interventions.Stat Med. 2019 Oct 30;38(24):4888-4911. doi: 10.1002/sim.8340. Epub 2019 Aug 22. Stat Med. 2019. PMID: 31436859 Free PMC article.
References
-
- Parkin DM. The role of cancer registries in cancer control. Int J Clin Oncol. 2008;13(2):102–111. - PubMed
-
- Siesling S, Louwman WJ, Kwast A, et al. . Uses of cancer registries for public health and clinical research in Europe: results of the European Network of Cancer Registries survey among 161 population-based cancer registries during 2010–2012. Eur J Cancer. 2015;51(9):1039–1049. - PubMed
-
- Andersson K, Bray F, Arbyn M, et al. . The interface of population-based cancer registries and biobanks in etiological and clinical research—current and future perspectives. Acta Oncol. 2010;49(8):1227–1234. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
