

Staging classification of aortic stenosis based on the extent of cardiac damage
- PMID: 29020232
- PMCID: PMC5837727
- DOI: 10.1093/eurheartj/ehx381
Staging classification of aortic stenosis based on the extent of cardiac damage
Abstract
Aims: In patients with aortic stenosis (AS), risk stratification for aortic valve replacement (AVR) relies mainly on valve-related factors, symptoms and co-morbidities. We sought to evaluate the prognostic impact of a newly-defined staging classification characterizing the extent of extravalvular (extra-aortic valve) cardiac damage among patients with severe AS undergoing AVR.
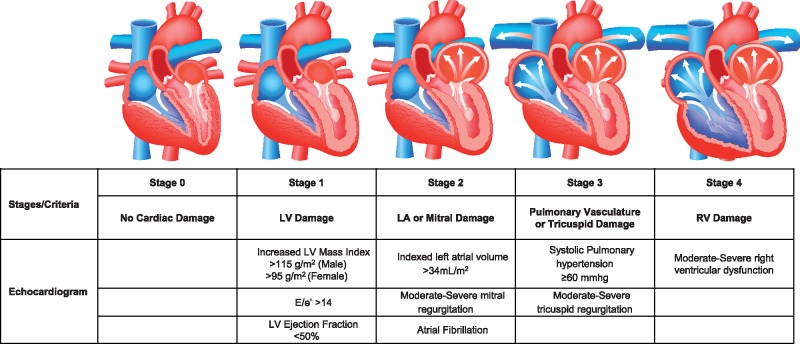
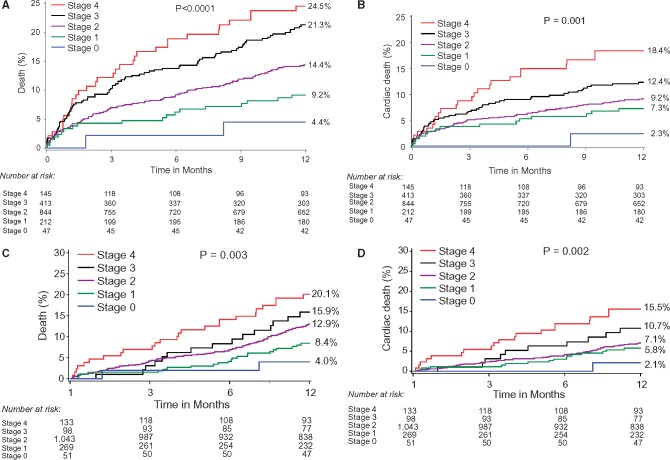
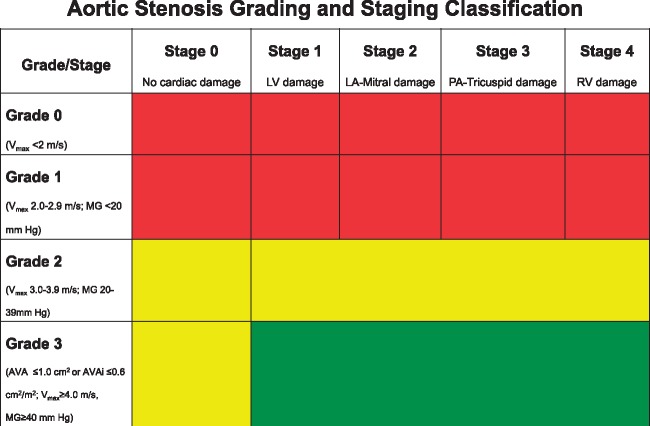
Methods and results: Patients with severe AS from the PARTNER 2 trials were pooled and classified according to the presence or absence of cardiac damage as detected by echocardiography prior to AVR: no extravalvular cardiac damage (Stage 0), left ventricular damage (Stage 1), left atrial or mitral valve damage (Stage 2), pulmonary vasculature or tricuspid valve damage (Stage 3), or right ventricular damage (Stage 4). One-year outcomes were compared using Kaplan-Meier techniques and multivariable Cox proportional hazards models were used to identify 1-year predictors of mortality. In 1661 patients with sufficient echocardiographic data to allow staging, 47 (2.8%) patients were classified as Stage 0, 212 (12.8%) as Stage 1, 844 (50.8%) as Stage 2, 413 (24.9%) as Stage 3, and 145 (8.7%) as Stage 4. One-year mortality was 4.4% in Stage 0, 9.2% in Stage 1, 14.4% in Stage 2, 21.3% in Stage 3, and 24.5% in Stage 4 (Ptrend < 0.0001). The extent of cardiac damage was independently associated with increased mortality after AVR (HR 1.46 per each increment in stage, 95% confidence interval 1.27-1.67, P < 0.0001).
Conclusion: This newly described staging classification objectively characterizes the extent of cardiac damage associated with AS and has important prognostic implications for clinical outcomes after AVR.
Keywords: Aortic stenosis; Aortic valve; Aortic valve replacement; Classification; Staging; Transcatheter aortic valve implantation; Transcatheter aortic valve replacement.
© The Author 2017. Published on behalf of the European Society of Cardiology.
Figures
Comment in
-
"Cardiac Damage" Predicts Prognosis, But Can It Identify Modifiable Prognosis?JACC Cardiovasc Imaging. 2022 Jun;15(6):1170-1173. doi: 10.1016/j.jcmg.2022.05.001. JACC Cardiovasc Imaging. 2022. PMID: 35680227 No abstract available.
References
-
- Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP 3rd, Guyton RA, O’Gara PT, Ruiz CE, Skubas NJ, Sorajja P, Sundt TM 3rd, Thomas JD; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014;63:2438–2488. - PubMed
-
- Vahanian A, Alfieri O, Andreotti F, Antunes MJ, Baron-Esquivias G, Baumgartner H, Borger MA, Carrel TP, De Bonis M, Evangelista A, Falk V, Iung B, Lancellotti P, Pierard L, Price S, Schafers HJ, Schuler G, Stepinska J, Swedberg K, Takkenberg J, Von Oppell UO, Windecker S, Zamorano JL, Zembala M.. Guidelines on the management of valvular heart disease (version 2012). Eur Heart J 2012;33:2451–2496. - PubMed
-
- Leon MB, Smith CR, Mack MJ, Makkar RR, Svensson LG, Kodali SK, Thourani VH, Tuzcu EM, Miller DC, Herrmann HC, Doshi D, Cohen DJ, Pichard AD, Kapadia S, Dewey T, Babaliaros V, Szeto WY, Williams MR, Kereiakes D, Zajarias A, Greason KL, Whisenant BK, Hodson RW, Moses JW, Trento A, Brown DL, Fearon WF, Pibarot P, Hahn RT, Jaber WA, Anderson WN, Alu MC, Webb JG; PARTNER 2 Investigators. Transcatheter or surgical aortic-valve replacement in intermediate-risk patients. N Engl J Med 2016;374:1609–1620. - PubMed
-
- Webb JG, Doshi D, Mack MJ, Makkar R, Smith CR, Pichard AD, Kodali S, Kapadia S, Miller DC, Babaliaros V, Thourani V, Herrmann HC, Bodenhamer M, Whisenant BK, Ramee S, Maniar H Jr, Kereiakes D, Xu K, Jaber WA, Menon V, Tuzcu EM, Wood D, Svensson LG, Leon MB.. A randomized evaluation of the SAPIEN XT transcatheter heart valve system in patients with aortic stenosis who are not candidates for surgery. JACC Cardiovasc Interv 2015;8:1797–1806. - PubMed
-
- Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, Flachskampf FA, Foster E, Goldstein SA, Kuznetsova T, Lancellotti P, Muraru D, Picard MH, Rietzschel ER, Rudski L, Spencer KT, Tsang W, Voigt JU.. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr 2015;28:1–39.e14. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
