

Antibiotic Expenditures by Medication, Class, and Healthcare Setting in the United States, 2010-2015
- PMID: 29020276
- PMCID: PMC9454312
- DOI: 10.1093/cid/cix773
Antibiotic Expenditures by Medication, Class, and Healthcare Setting in the United States, 2010-2015
Abstract
Background: Improving antibiotic use has the potential to decrease healthcare costs by reducing the incidence of antibiotic-resistant infections, antibiotic-associated adverse events, and expenditures due to unnecessary prescriptions. Antibiotic expenditures in 2009 totaled $10.7 billion in the United States. Since then, national and local antibiotic stewardship initiatives have grown. The purpose of this study was to assess trends in antibiotic expenditures by healthcare setting in the United States between 2010 and 2015.
Methods: Systemic (nontopical) antibiotic expenditures from January 2010 to December 2015 were extracted from the QuintilesIMS National Sales Perspectives database. These data represent a statistically valid projection of US medication purchases. Regression analyses evaluated trends in expenditures over the study period.
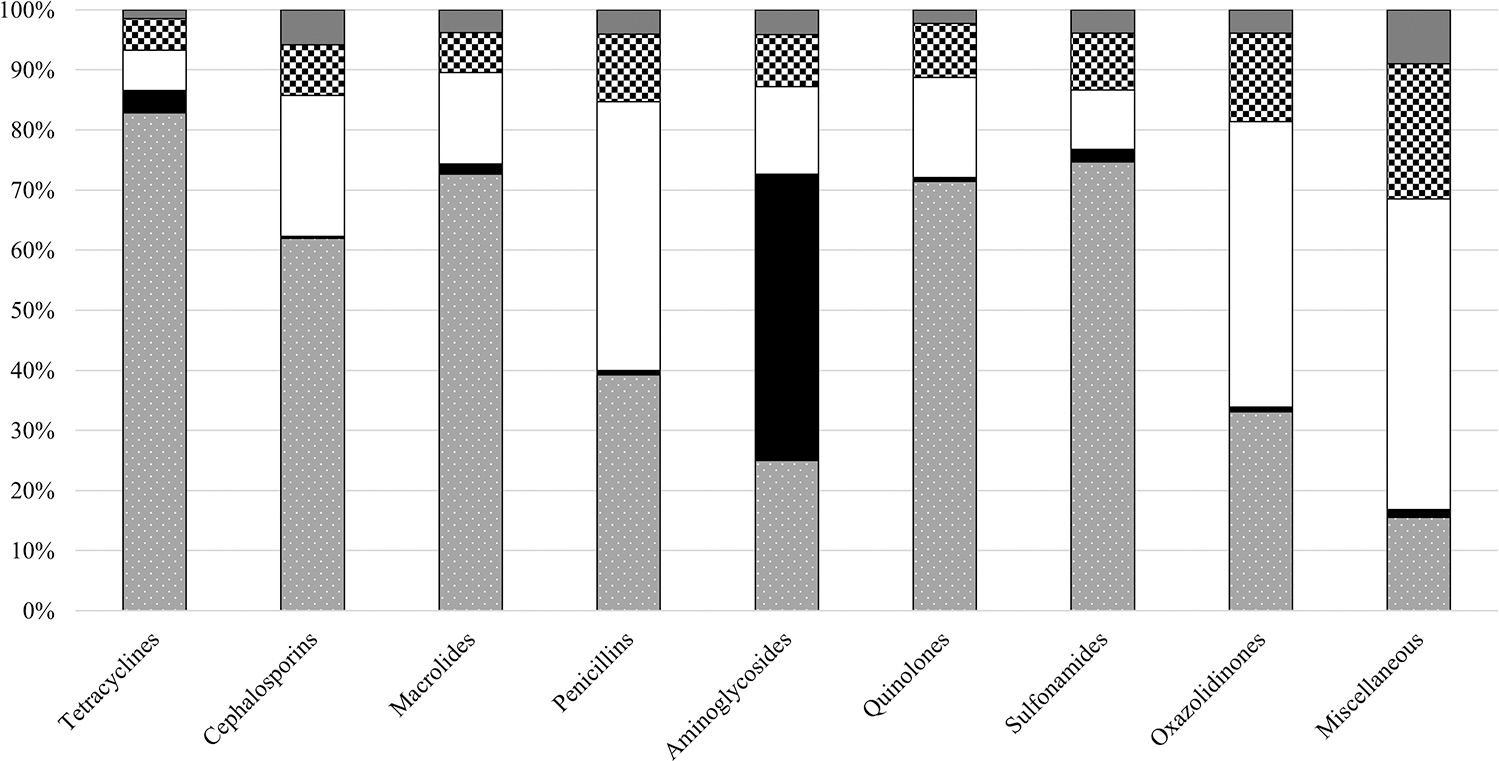
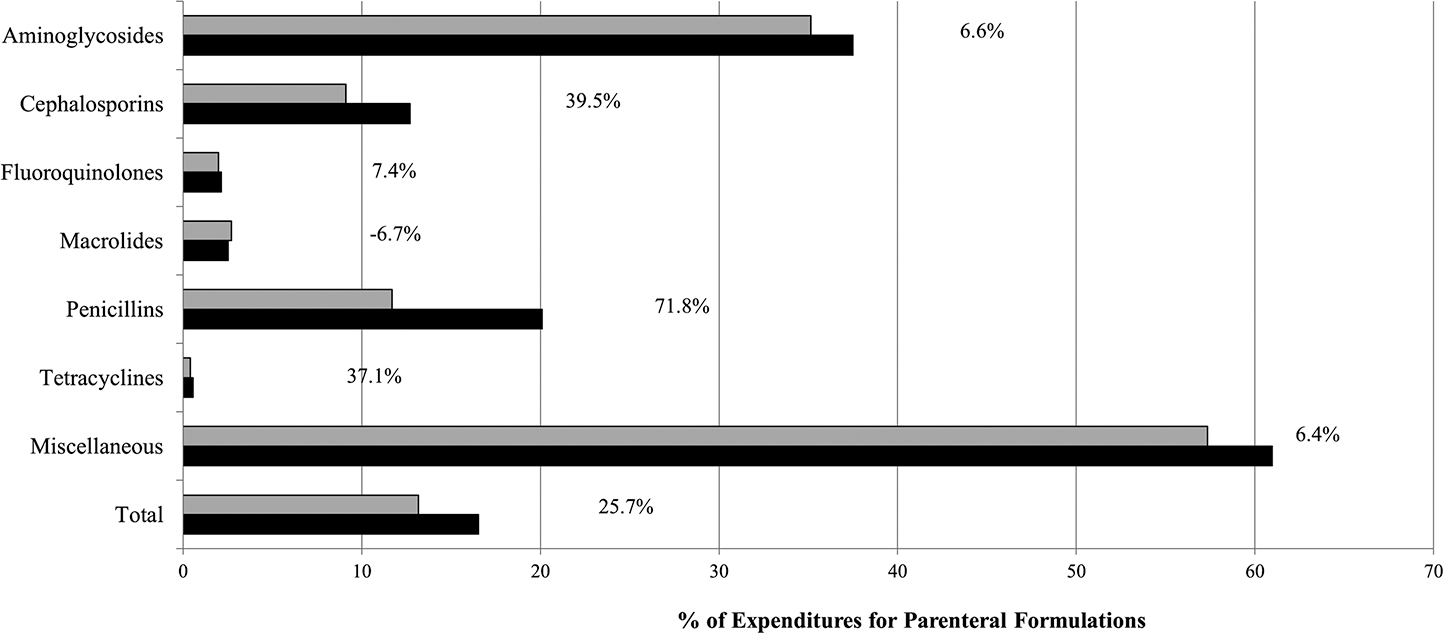
Results: Antibiotic expenditures totaled $56.0 billion over the 6-year period; the majority (59.1%) of expenditures were associated with the outpatient setting. Overall antibiotic expenditures in 2015 ($8.8 billion) were 16.6% lower than in 2010 ($10.6 billion). Antibiotic expenditures similarly decreased in the community by 25.5% (P = .05), but outpatient clinics and mail service pharmacy expenditures experienced significant growth (148% and 67% increase, respectively; P < .01 for both). In 2015, 16.5% of antibiotic expenditures in the community were for parenteral formulations, an increase of 25%.
Conclusions: From 2010 to 2015, antibiotic expenditures decreased. The majority of antibiotic expenditures were in the outpatient setting, specifically community pharmacies. Expenditures for intravenous agents in the community are increasing and may represent increased use. These results reinforce the importance of antibiotic stewardship efforts across the spectrum of healthcare.
Keywords: antibiotic; community; expenditures; outpatient parenteral antimicrobial therapy; stewardship.
Published by Oxford University Press for the Infectious Diseases Society of America 2017. This work is written by (a) US Government employee(s) and is in the public domain in the US.
Conflict of interest statement
Figures
References
-
- Davey P, Brown E, Charani E, et al. Interventions to improve antibiotic prescribing practices for hospital inpatients. Cochrane Database Syst Rev 2013; 4:CD003543. - PubMed
-
- Filice G, Drekonja D, Greer N, et al. Antimicrobial stewardship programs in inpatient settings: a systematic review. VA-ESP Project #09-009. Washington, DC: Department of Veterans Affairs, 2013. - PubMed
-
- Fleming-Dutra KE, Hersh AL, Shapiro DJ, et al. Prevalence of inappropriate antibiotic prescriptions among U.S. ambulatory care visits, 2010–2011. JAMA 2016; 315:1864–73. - PubMed
-
- Hecker MT, Aron DC, Patel NP, Lehmann MK, Donskey CJ. Unnecessary use of antimicrobials in hospitalized patients: current patterns of misuse with an emphasis on the antianaerobic spectrum of activity. Arch Intern Med 2003; 163:972–8. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
