

Impact of Systemic Antibiotics on Staphylococcus aureus Colonization and Recurrent Skin Infection
- PMID: 29020285
- PMCID: PMC5850557
- DOI: 10.1093/cid/cix754
Impact of Systemic Antibiotics on Staphylococcus aureus Colonization and Recurrent Skin Infection
Abstract
Background: Staphylococcus aureus colonization poses risk for subsequent skin and soft tissue infection (SSTI). We hypothesized that including systemic antibiotics in the management of S. aureus SSTI, in conjunction with incision and drainage, would reduce S. aureus colonization and incidence of recurrent infection.
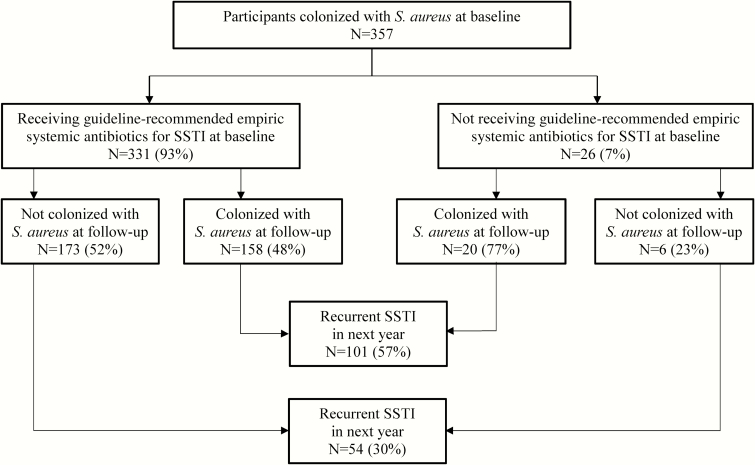
Methods: We prospectively evaluated 383 children with S. aureus SSTI requiring incision and drainage and S. aureus colonization in the anterior nares, axillae, or inguinal folds at baseline screening. Systemic antibiotic prescribing at the point of care was recorded. Repeat colonization sampling was performed within 3 months (median, 38 days; interquartile range, 22-50 days) in 357 participants. Incidence of recurrent infection was ascertained for up to 1 year.
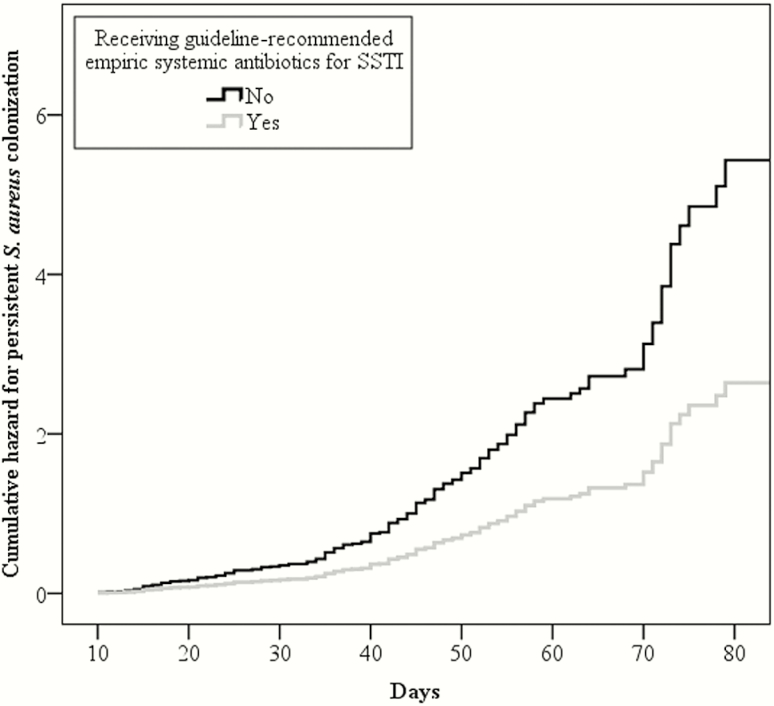
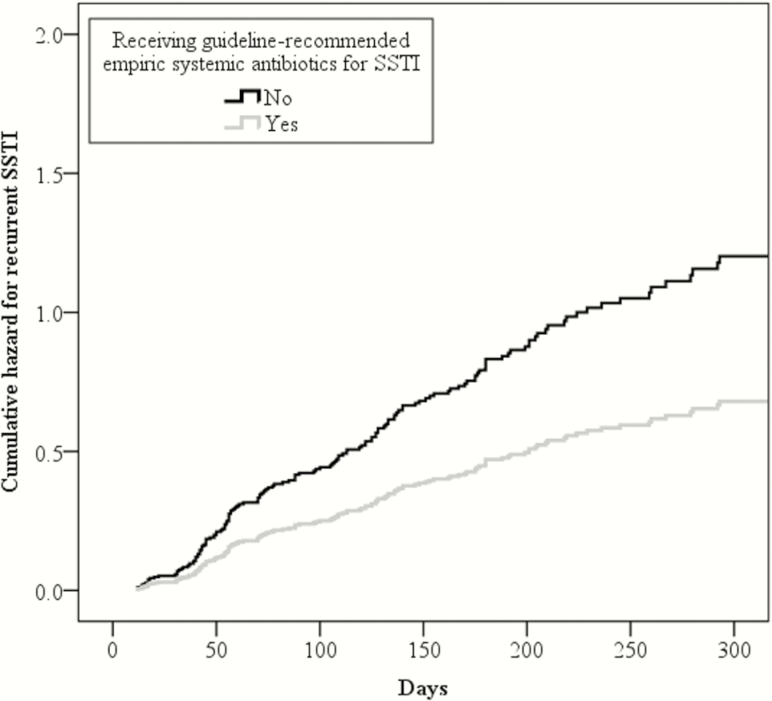
Results: Participants prescribed guideline-recommended empiric antibiotics for purulent SSTI were less likely to remain colonized at follow-up sampling (adjusted hazard ratio [aHR], 0.49; 95% confidence interval [CI], .30-.79) and less likely to have recurrent SSTI (aHR, 0.57; 95% CI, .34-.94) than those not receiving guideline-recommended empiric antibiotics for their SSTI. Additionally, participants remaining colonized at repeat sampling were more likely to report a recurrent infection over 12 months (aHR, 2.37; 95% CI, 1.69-3.31). Clindamycin was more effective than trimethoprim-sulfamethoxazole (TMP-SMX) in eradicating S. aureus colonization (44% vs 57% remained colonized, P = .03) and preventing recurrent SSTI (31% vs 47% experienced recurrence, P = .008).
Conclusions: Systemic antibiotics, as part of acute SSTI management, impact S. aureus colonization, contributing to a decreased incidence of recurrent SSTI. The mechanism by which clindamycin differentially affects colonization and recurrent SSTI compared to TMP-SMX warrants further study.
Keywords: SSTI; Staphylococcus aureus; colonization; systemic antibiotics.
© The Author 2017. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
References
-
- Hersh AL, Chambers HF, Maselli JH, Gonzales R. National trends in ambulatory visits and antibiotic prescribing for skin and soft-tissue infections. Arch Intern Med 2008; 168:1585–91. - PubMed
-
- Witt WP, Weiss AJ, Elixhauser A.. Overview of hospital stays for children in the United States, 2012. Healthcare Cost and Utilization Project (HCUP) statistical brief No. 187. Rockville, MD:Agency for Healthcare Research and Quality, 2014. Available at: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb187-Hospital-Stays-Chil.... Accessed 14 April 2017. - PubMed
-
- Kaplan SL. Community-acquired methicillin-resistant Staphylococcus aureus infections in children. Semin Pediatr Infect Dis 2006; 17:113–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
