

Impaired β-Oxidation and Altered Complex Lipid Fatty Acid Partitioning with Advancing CKD
- PMID: 29021384
- PMCID: PMC5748913
- DOI: 10.1681/ASN.2017030350
Impaired β-Oxidation and Altered Complex Lipid Fatty Acid Partitioning with Advancing CKD
Abstract
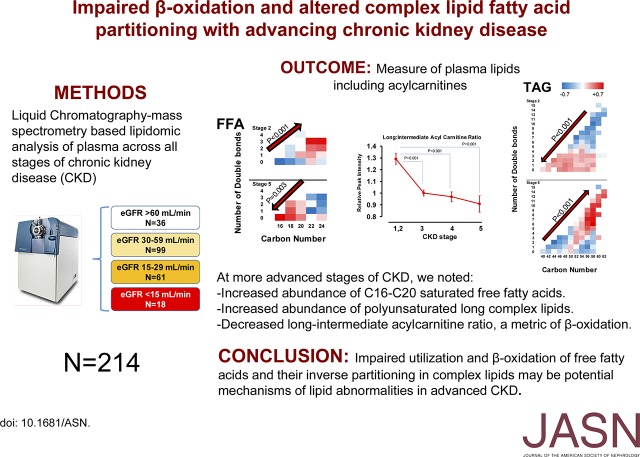
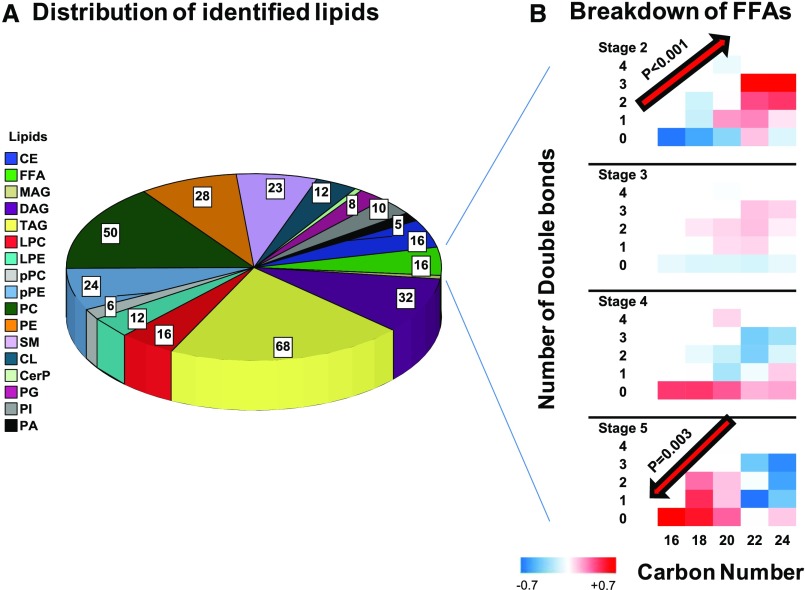
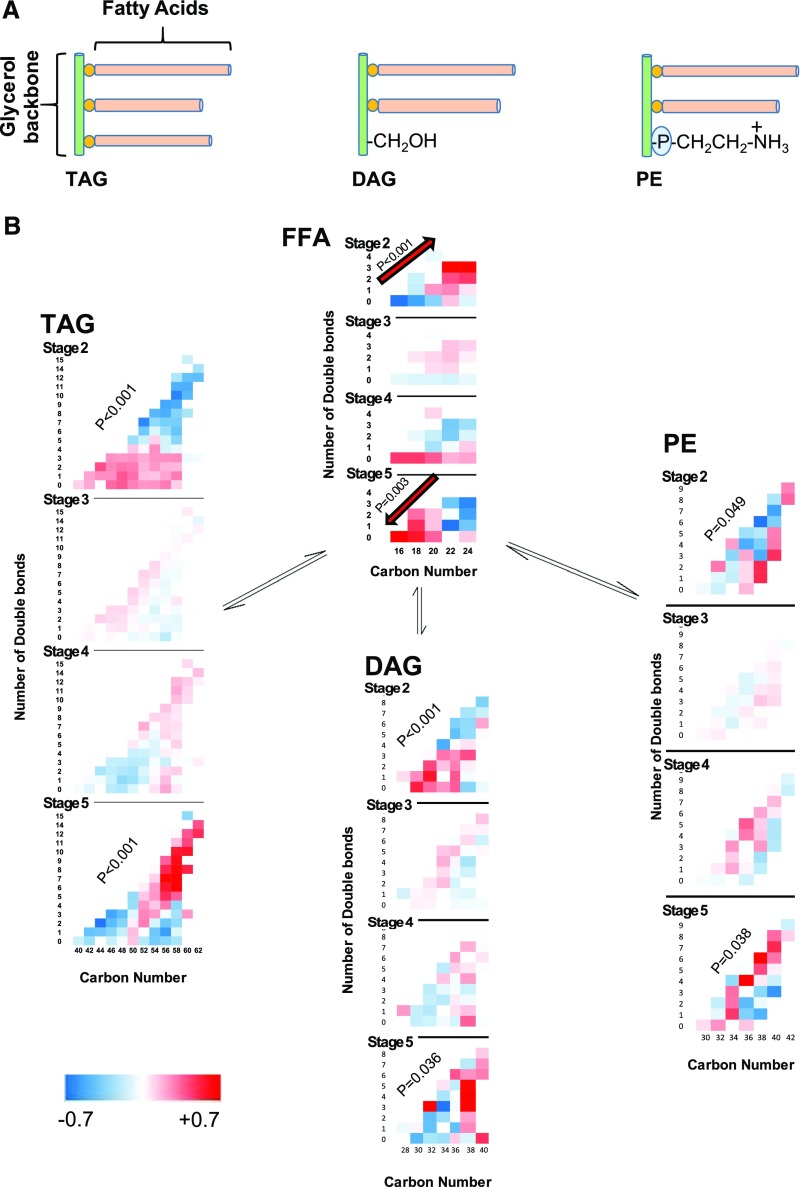
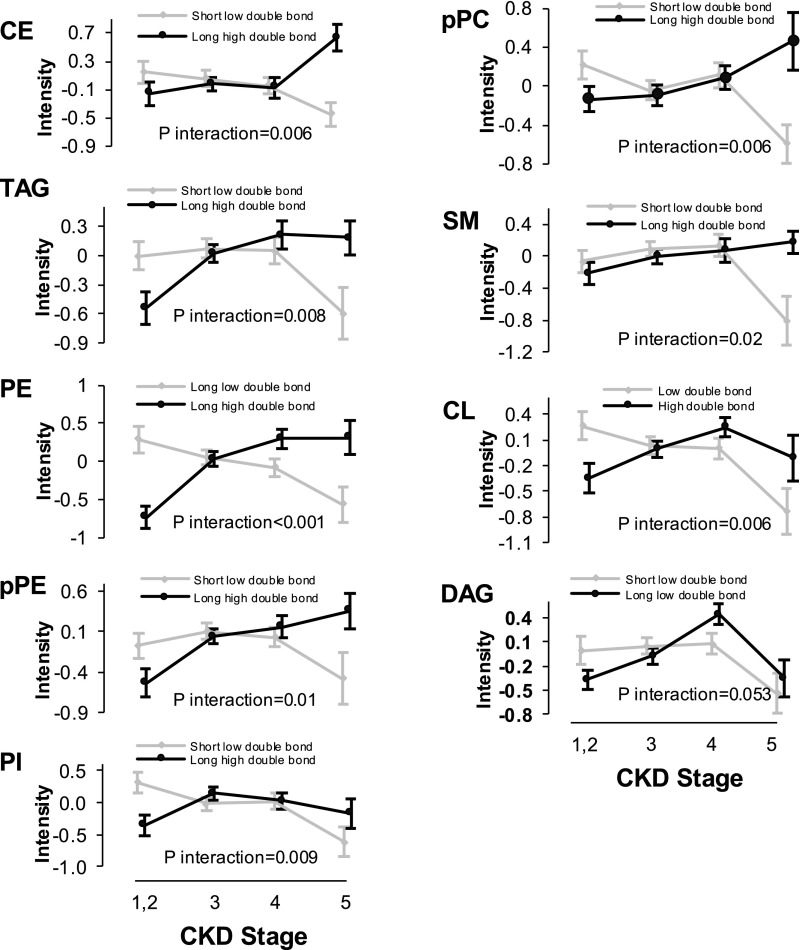
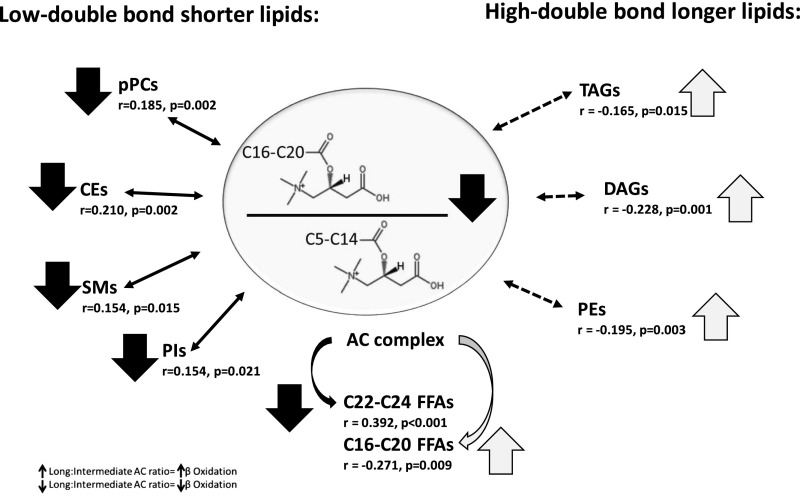
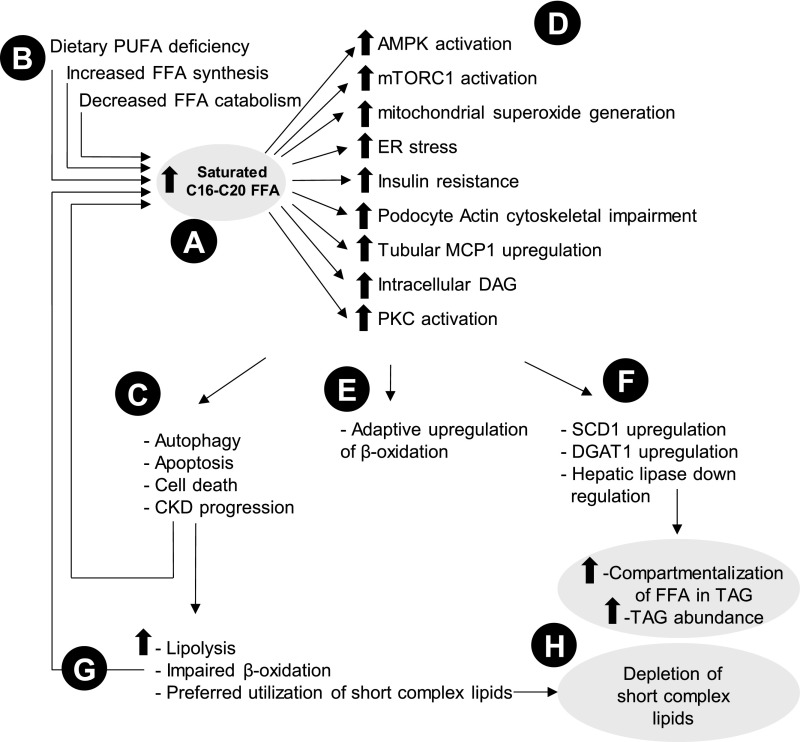
Studies of lipids in CKD, including ESRD, have been limited to measures of conventional lipid profiles. We aimed to systematically identify 17 different lipid classes and associate the abundance thereof with alterations in acylcarnitines, a metric of β-oxidation, across stages of CKD. From the Clinical Phenotyping Resource and Biobank Core (CPROBE) cohort of 1235 adults, we selected a panel of 214 participants: 36 with stage 1 or 2 CKD, 99 with stage 3 CKD, 61 with stage 4 CKD, and 18 with stage 5 CKD. Among participants, 110 were men (51.4%), 64 were black (29.9%), and 150 were white (70.1%), and the mean (SD) age was 60 (16) years old. We measured plasma lipids and acylcarnitines using liquid chromatography-mass spectrometry. Overall, we identified 330 different lipids across 17 different classes. Compared with earlier stages, stage 5 CKD associated with a higher abundance of saturated C16-C20 free fatty acids (FFAs) and long polyunsaturated complex lipids. Long-chain-to-intermediate-chain acylcarnitine ratio, a marker of efficiency of β-oxidation, exhibited a graded decrease from stage 2 to 5 CKD (P<0.001). Additionally, multiple linear regression revealed that the long-chain-to-intermediate-chain acylcarnitine ratio inversely associated with polyunsaturated long complex lipid subclasses and the C16-C20 FFAs but directly associated with short complex lipids with fewer double bonds. We conclude that increased abundance of saturated C16-C20 FFAs coupled with impaired β-oxidation of FFAs and inverse partitioning into complex lipids may be mechanisms underpinning lipid metabolism changes that typify advancing CKD.
Keywords: Acylcarnitines; Free fatty acids; chronic kidney disease; complex lipids; lipids.
Copyright © 2018 by the American Society of Nephrology.
Figures

References
-
- Attman PO, Alaupovic P: Lipid abnormalities in chronic renal insufficiency. Kidney Int Suppl 31: S16–S23, 1991 - PubMed
-
- Trevisan R, Dodesini AR, Lepore G: Lipids and renal disease. J Am Soc Nephrol 17[Suppl 2]: S145–S147, 2006 - PubMed
-
- Longenecker JC, Coresh J, Powe NR, Levey AS, Fink NE, Martin A, Klag MJ: Traditional cardiovascular disease risk factors in dialysis patients compared with the general population: The CHOICE Study. J Am Soc Nephrol 13: 1918–1927, 2002 - PubMed
-
- Pennell P, Leclercq B, Delahunty MI, Walters BA: The utility of non-HDL in managing dyslipidemia of stage 5 chronic kidney disease. Clin Nephrol 66: 336–347, 2006 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
