

Modeling of Antilatency Treatment in HIV: What Is the Optimal Duration of Antiretroviral Therapy-Free HIV Remission?
- PMID: 29021399
- PMCID: PMC5709587
- DOI: 10.1128/JVI.01395-17
Modeling of Antilatency Treatment in HIV: What Is the Optimal Duration of Antiretroviral Therapy-Free HIV Remission?
Abstract
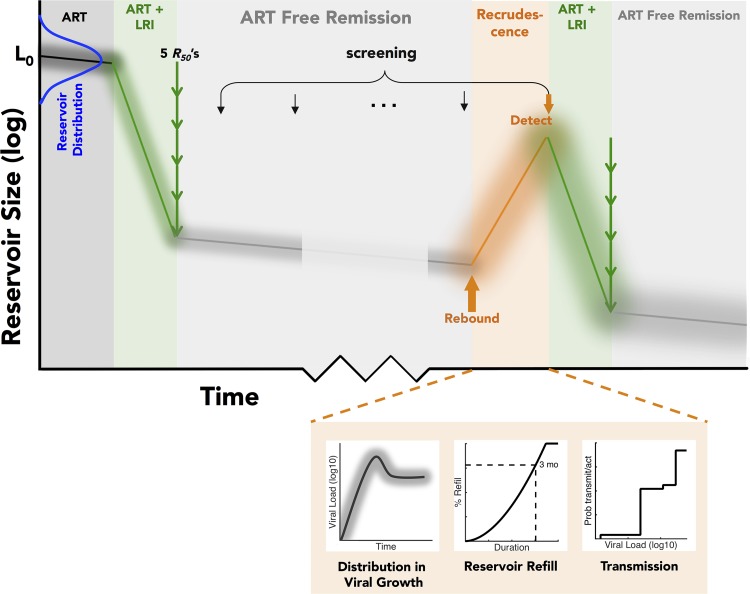
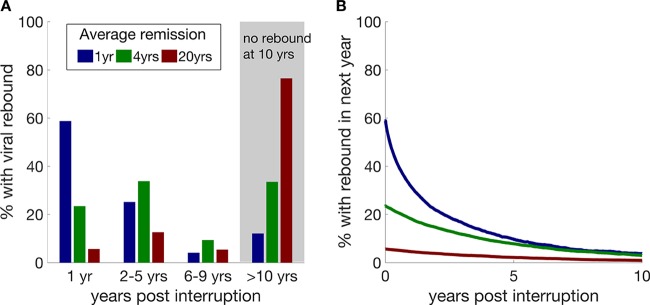
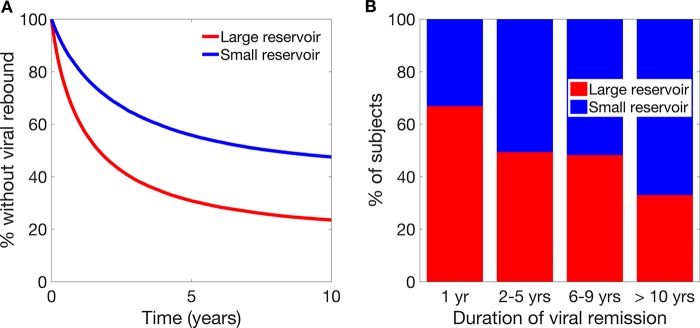
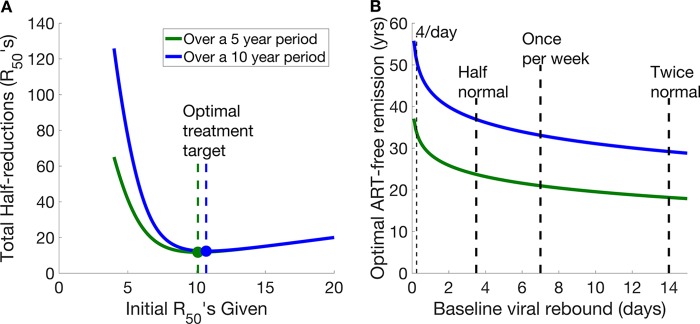
A number of treatment strategies are currently being developed to promote antiretroviral therapy-free HIV cure or remission. While complete elimination of the HIV reservoir would prevent recurrence of infection, it is not clear how different remission lengths would affect viral rebound and transmission. In this work, we use a stochastic model to show that a treatment that achieves a 1-year average time to viral remission will still lead to nearly a quarter of subjects experiencing viral rebound within the first 3 months. Given quarterly viral testing intervals, this leads to an expected 39 (95% uncertainty interval [UI], 22 to 69) heterosexual transmissions and up to 262 (95% UI, 107 to 534) homosexual transmissions per 1,000 treated subjects over a 10-year period. Thus, a balance between high initial treatment levels, risk of recrudescence, and risk of transmission should be considered when assessing the "useful" or optimal length of antiretroviral therapy-free HIV remission to be targeted. We also investigate the trade-off between increasing the average duration of remission versus the risk of treatment failure (viral recrudescence) and the need for retreatment. To minimize drug exposure, we found that the optimal target of antilatency interventions is a 1,700-fold reduction in the size of the reservoir, which leads to an average time to recrudescence of 30 years. Interestingly, this is a significantly lower level of reduction than that required for complete elimination of the viral reservoir. Additionally, we show that when shorter periods are targeted, there is a real probability of viral transmission occurring between tests for viral rebound.IMPORTANCE Current treatment of HIV involves patients taking antiretroviral therapy to ensure that the level of virus remains very low or undetectable. Continuous therapy is required, as the virus persists in a latent state within cells, and when therapy is stopped, the virus rebounds, usually within 2 weeks. A major question is how to reduce the amount of persistent virus and therefore allow a delay or remission until the virus returns after ceasing therapy. In this work, we consider the probability that HIV will still rebound even after this reduction and ask what the likelihood of viral transmission would be in this case.
Keywords: HIV; latency; reactivation; remission.
Copyright © 2017 American Society for Microbiology.
Figures
References
-
- Deeks SG, Lewin SR, Ross AL, Ananworanich J, Benkirane M, Cannon P, Chomont N, Douek D, Lifson JD, Lo Y-R, Kuritzkes D, Margolis D, Mellors J, Persaud D, Tucker JD, Barre-Sinoussi F, International AIDS Society Towards a Cure Working Group, Alter G, Auerbach J, Autran B, Barouch DH, Behrens G, Cavazzana M, Chen Z, Cohen ÉA, Corbelli GM, Eholié S, Eyal N, Fidler S, Garcia L, Grossman C, Henderson G, Henrich TJ, Jefferys R, Kiem H-P, McCune J, Moodley K, Newman PA, Nijhuis M, Nsubuga MS, Ott M, Palmer S, Richman D, Saez-Cirion A, Sharp M, Siliciano J, Silvestri G, Singh J, Spire B, Taylor J, Tolstrup M, Valente S, van Lunzen J, Walensky R, Wilson I, Zack J. 2016. International AIDS Society global scientific strategy: towards an HIV cure 2016. Nat Med 22:839–850. doi:10.1038/nm.4108. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
