

A very rare spinal cord tumor primary spinal oligodendroglioma: A review of sixty cases in the literature
- PMID: 29021677
- PMCID: PMC5634112
- DOI: 10.4103/jcvjs.JCVJS_1_17
A very rare spinal cord tumor primary spinal oligodendroglioma: A review of sixty cases in the literature
Abstract
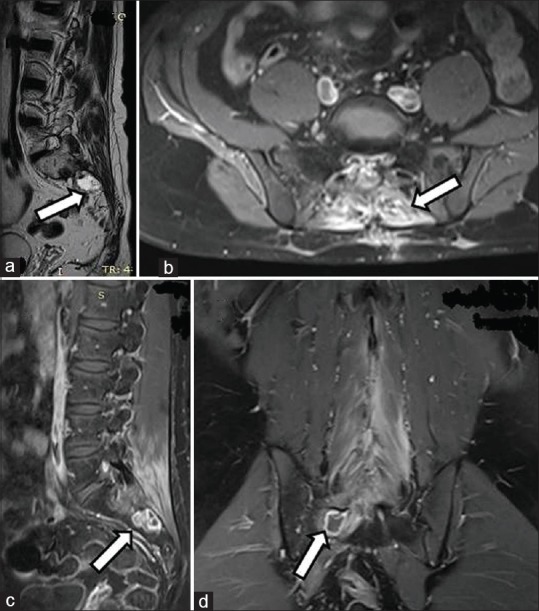
In this study, we evaluated a case of primary spinal oligodendroglioma (PSO) with a rare localization between L3 and S2, and also examined sixty cases in the literature in terms of demographic characteristics, clinical, radiological, and histopathological characteristics, and treatment planning. A case of PSO has been presented, and the relevant literature between 1931 and 2016 was reviewed. A total of 57 papers regarding PSO were found and utilized in this review. The main treatment options include radical surgical excision with neuromonitoring, followed by radiotherapy. Despite these treatment protocols, the relapse rate is high, and treatment does not significantly prolong survival. Oligodendrogliomas are rare among the primary spinal cord tumors. Oligodendrogliomas are predominantly found in the cervical spinal cord, thoracic spinal cord, or junctions during childhood and adulthood. Extension to the sacral region, inferior to the Conus, is very rare. Furthermore, of the sixty cases in the literature, the case we present here is the first to be reported in this particular age group. These localizations usually occur in the pediatric age group and after relapses. While for a limited number of cases the oligodendroglioma initiates in the thoracic region and reaches as far as L2, we encountered a case of an oligodendroglioma within the range of L3 to S2. Clinical findings are observed in accordance with location, and magnetic resonance imaging is the gold standard for diagnosis.
Keywords: Management; primary spinal oligodendroglioma; review.
Conflict of interest statement
There are no conflicts of interest.
Figures




References
-
- Tunthanathip T, Oearsakul T. Primary spinal cord oligodendroglioma: A case report and review of the literature. Chin Neurosurg J. 2016;2:2.
-
- Moorthy NL, Kondeti D, Chander M, Jadhav H, Ashok Spinal cord oligodendroglioma: A case report. IOSR J Dent Med Sci. 2015;14:27–8.
-
- Wang F, Qiao G, Lou X. Spinal cord anaplastic oligodendroglioma with 1p deletion: Report of a relapsing case treated with temozolomide. J Neurooncol. 2011;104:387–94. - PubMed
-
- Guppy KH, Akins PT, Moes GS, Prados MD. Spinal cord oligodendroglioma with 1p and 19q deletions presenting with cerebral oligodendrogliomatosis. J Neurosurg Spine. 2009;10:557–63. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
