

Continuous Curvilinear Capsulorhexis Training and Non-Rhexis Related Vitreous Loss: The Specificity of Virtual Reality Simulator Surgical Training (An American Ophthalmological Society Thesis)
- PMID: 29021716
- PMCID: PMC5598788
Continuous Curvilinear Capsulorhexis Training and Non-Rhexis Related Vitreous Loss: The Specificity of Virtual Reality Simulator Surgical Training (An American Ophthalmological Society Thesis)
Abstract
Purpose: To assess the specificity of simulation-based virtual reality ophthalmic cataract surgery training on the Eyesi ophthalmic virtual reality surgical simulator, and test the hypothesis that microsurgical motor learning is highly specific.
Methods: Retrospective educational interventional case series. The rates of vitreous loss and retained lens material, and vitreous loss and retained lens material associated with an errant continuous curvilinear capsulorhexis (CCC) were assessed among 1037 consecutive cataract surgeries performed during four consecutive academic years at a teaching hospital. The data were grouped by Eyesi use and capsulorhexis intensive training curriculum (CITC) completion. The main intervention was the completion of the CITC on the Eyesi.
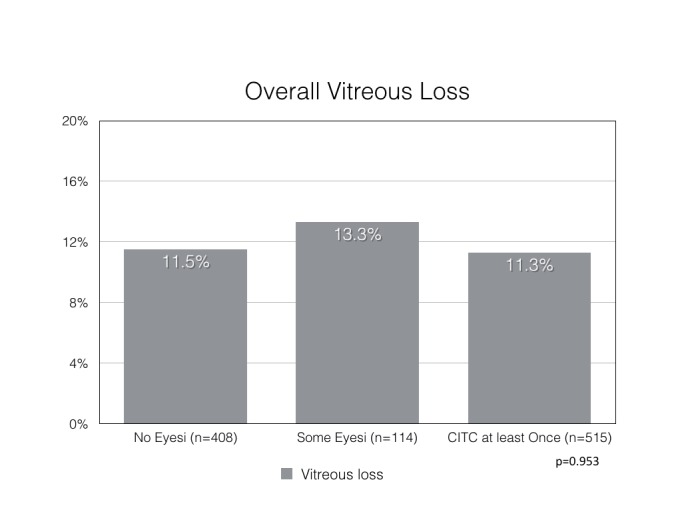
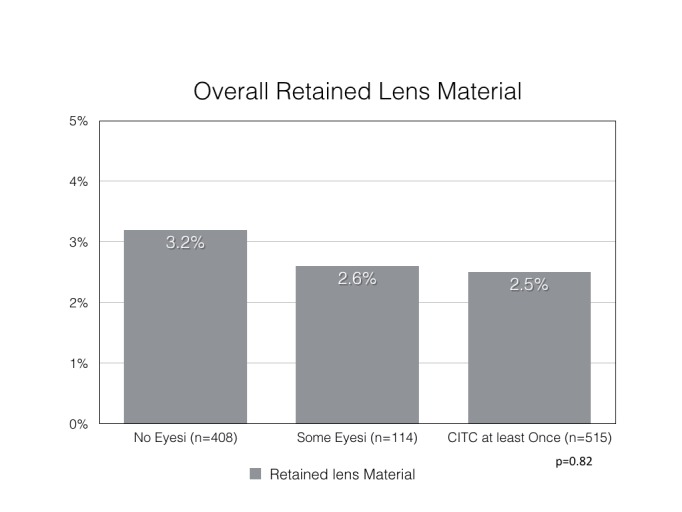
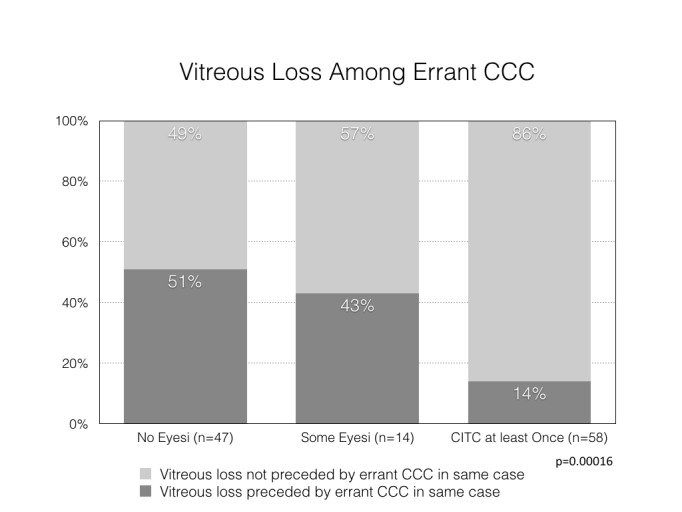
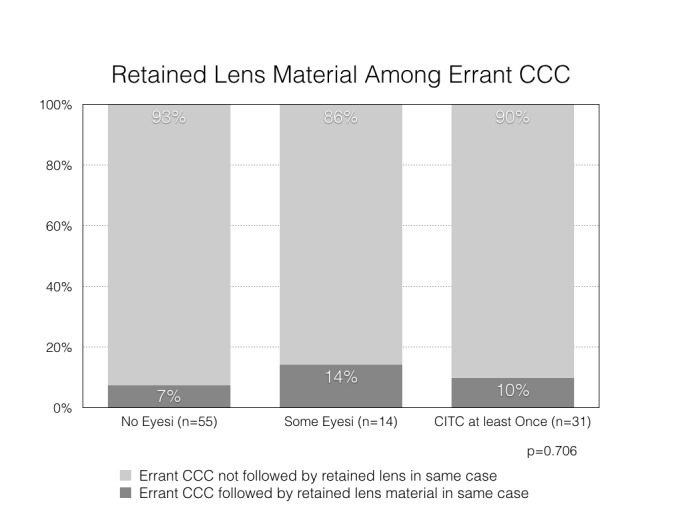
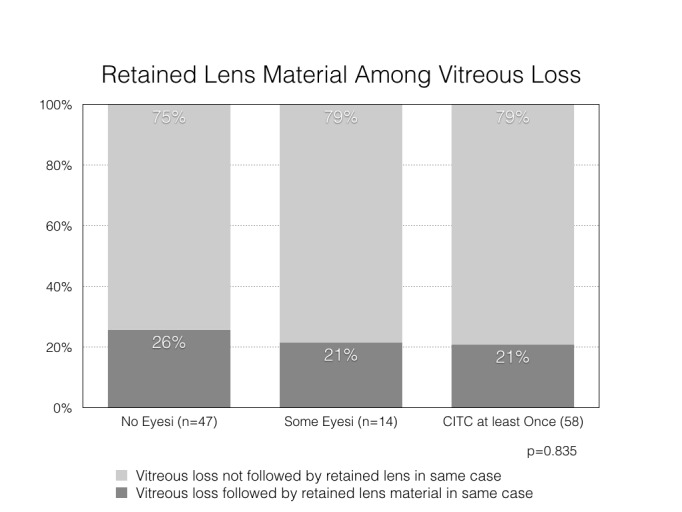
Results: In the Eyesi simulator experience-based stratification, the vitreous loss rate was similar in each group (chi square p=0.95) and was not preceded by an errant CCC in 86.2% for "CITC done at least once", 57.1% for "CITC not done, but some Eyesi use", and 48.9% for "none" training groups (p=4×10-5). Retained lens material overall and occurring among the errant CCC cases was similar among training groups (p=0.82 and p=0.71, respectively).
Conclusions: Eyesi capsulorhexis training was not associated with lower vitreous loss rates overall. However, non-errant CCC associated vitreous loss was higher among those who underwent Eyesi capsulorhexis training. Training focused on the CCC portion of cataract surgery may not reduce vitreous loss unassociated with an errant CCC. It is likely that surgical training is highly specific to the task being trained. Residents may need to be trained for all surgical steps with adequate intensity to minimize overall complication rates.
Figures
References
-
- Noecker RJ, Allinson RW, Snyder RW. Resident phacoemulsification experience using the in situ nuclear fracture technique. Ophthalmic Surg. 1994;25:216–221. - PubMed
-
- Tarbet KJ, Mamalis N, Theurer J, Jones BD, Olson RJ. Complications and results of phacoemulsification performed by residents. J Cataract Refract Surg. 1995;21:661–665. - PubMed
-
- Corey RP, Olson RJ. Surgical outcomes of cataract extractions performed by residents using phacoemulsification. J Cataract Refract Surg. 1998;24:66–72. - PubMed
-
- Blomquist PH, Rugwani RM. Visual outcomes after vitreous loss during cataract surgery performed by residents. J Cataract Refract Surg. 2002;28(5):847–52. - PubMed
-
- Tan JH, Karwatowski WS. Phacoemulsification cataract surgery and unplanned anterior vitrectomy--is it bad news?[see comment] Eye. 2002;16(2):117–20. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical