

Sex Differences in rt-PA Utilization at Hospitals Treating Stroke: The National Inpatient Sample
- PMID: 29021776
- PMCID: PMC5623663
- DOI: 10.3389/fneur.2017.00500
Sex Differences in rt-PA Utilization at Hospitals Treating Stroke: The National Inpatient Sample
Abstract
Background and purpose: Sex and race disparities in recombinant tissue plasminogen activator (rt-PA) use have been reported. We sought to explore sex and race differences in the utilization of rt-PA at primary stroke centers (PSCs) compared to non-PSCs across the US.
Methods: Data from the National (Nationwide) Inpatient Sample (NIS) 2004-2010 was utilized to assess sex differences in treatment for ischemic stroke in PSCs compared to non-PSCs.
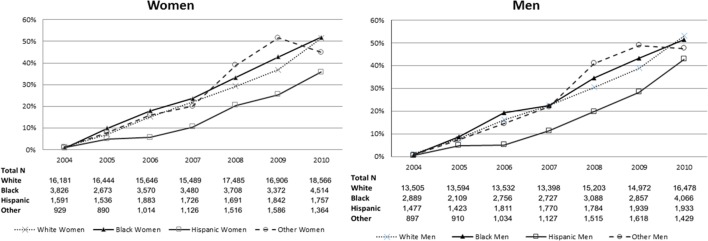
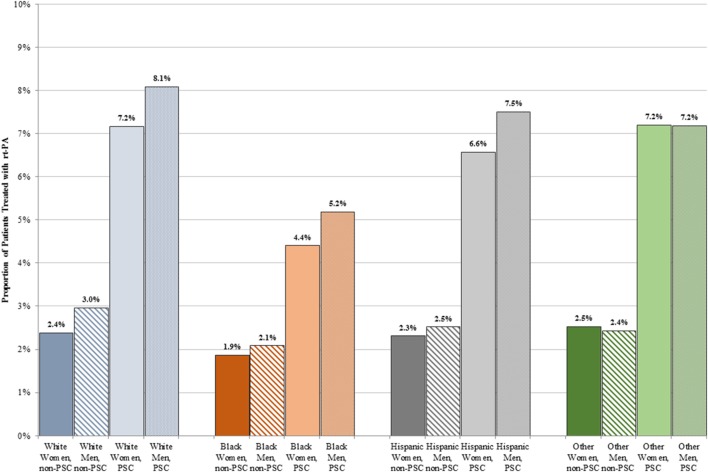
Results: There were 304,152 hospitalizations with a primary diagnosis of ischemic stroke between 2004 and 2010 in the analysis: 75,160 (24.7%) patients were evaluated at a PSC. A little over half of the patients evaluated at PSCs were female (53.8%). A lower proportion of women than men received rt-PA at both PSCs (6.8 vs. 7.5%, p < 0.001) and non-PSCs (2.3 vs. 2.8%, p < 0.001). After adjustment for potential confounders the odds of being treated with rt-PA remained lower for women regardless of presentation to a PSC (OR 0.87, 95% CI 0.81-0.94) or non-PSC (OR 0.88, 95% CI 0.82-0.94). After stratifying by sex and race, the lowest absolute treatment rates were observed in black women (4.4% at PSC, 1.9% at non-PSC). The odds of treatment, relative to white men, was however lowest for white women (PSC OR = 0.85, 95% CI 0.78-0.93; non-PSC OR = 0.80, 95% CI 0.75-0.85). In the multivariable model, sex did not modify the effect of PSC certification on rt-PA utilization (p-value for interaction = 0.58).
Conclusion: Women are less likely to receive rt-PA than men at both PSCs and non-PSCs. Absolute treatment rates are lowest in black women, although the relative difference in men and women was greatest for white women.
Keywords: acute stroke care; emergency care; health policy; healthcare delivery systems; thrombolysis.
Figures
References
-
- Del Zoppo GJ, Saver JL, Jauch EC, Adams HP, Council AHAS Expansion of the time window for treatment of acute ischemic stroke with intravenous tissue plasminogen activator: a science advisory from the American Heart Association/American Stroke Association. Stroke (2009) 40:2945–8. 10.1161/STROKEAHA.109.192535 - DOI - PMC - PubMed
-
- Schwamm LH, Ali SF, Reeves MJ, Smith EE, Saver JL, Messe S, et al. Temporal trends in patient characteristics and treatment with intravenous thrombolysis among acute ischemic stroke patients at get with the guidelines-stroke hospitals. Circ Cardiovasc Qual Outcomes (2013) 6:543–9. 10.1161/CIRCOUTCOMES.111.000303 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources