

Cross Talk between Adipose Tissue and Placenta in Obese and Gestational Diabetes Mellitus Pregnancies via Exosomes
- PMID: 29021781
- PMCID: PMC5623931
- DOI: 10.3389/fendo.2017.00239
Cross Talk between Adipose Tissue and Placenta in Obese and Gestational Diabetes Mellitus Pregnancies via Exosomes
Abstract
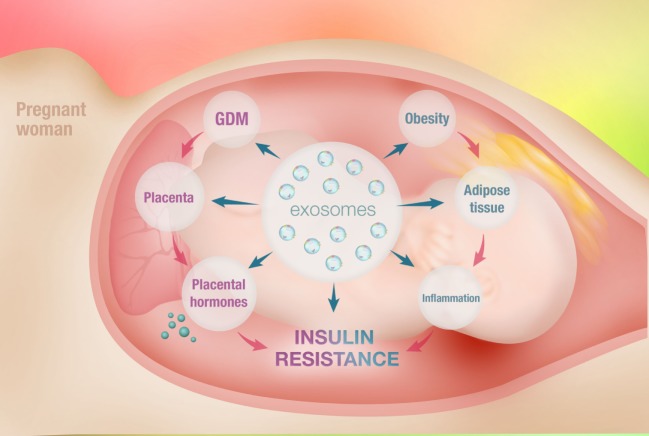
Obesity is an important public health issue worldwide, where it is commonly associated with the development of metabolic disorders, especially insulin resistance (IR). Maternal obesity is associated with an increased risk of pregnancy complications, especially gestational diabetes mellitus (GDM). Metabolism is a vital process for energy production and the maintenance of essential cellular functions. Excess energy storage is predominantly regulated by the adipose tissue. Primarily made up of adipocytes, adipose tissue acts as the body's major energy reservoir. The role of adipose tissue, however, is not restricted to a "bag of fat." The adipose tissue is an endocrine organ, secreting various adipokines, enzymes, growth factors, and hormones that take part in glucose and lipid metabolism. In obesity, the greater portion of the adipose tissue comprises fat, and there is increased pro-inflammatory cytokine secretion, macrophage infiltration, and reduced insulin sensitivity. Obesity contributes to systemic IR and its associated metabolic complications. Similar to adipose tissue, the placenta is also an endocrine organ. During pregnancy, the placenta secretes various molecules to maintain pregnancy physiology. In addition, the placenta plays an important role in metabolism and exchange of nutrients between mother and fetus. Inflammation at the placenta may contribute to the severity of maternal IR and her likelihood of developing GDM and may also mediate the adverse consequences of obesity and GDM on the fetus. Interestingly, studies on maternal insulin sensitivity and secretion of placental hormones have not shown a positive correlation between these phenomena. Recently, a great interest in the field of extracellular vesicles (EVs) has been observed in the literature. EVs are produced by a wide range of cells and are present in all biological fluids. EVs are involved in cell-to-cell communication. Recent evidence points to an association between adipose tissue-derived EVs and metabolic syndrome in obesity. In this review, we will discuss the changes in human placenta and adipose tissue in GDM and obesity and summarize the findings regarding the role of adipose tissue and placenta-derived EVs, with an emphasis on exosomes in obesity, and the contribution of obesity to the development of GDM.
Keywords: adipose tissue; adipose tissue-derived exosomes; extracellular vesicles; gestational diabetes; obesity.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources