

Disease modification and Neuroprotection in neurodegenerative disorders
- PMID: 29021896
- PMCID: PMC5613313
- DOI: 10.1186/s40035-017-0096-2
Disease modification and Neuroprotection in neurodegenerative disorders
Abstract
Background: Disease modifying therapies (DMTs) are urgently needed for neurodegenerative diseases (NDD) such as Alzheimer's disease (AD) and many other disorders characterized by protein aggregation and neurodegeneration. Despite advances in understanding the neurobiology of NDD, there are no approved DMTs.
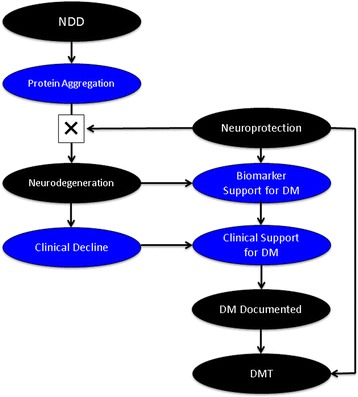
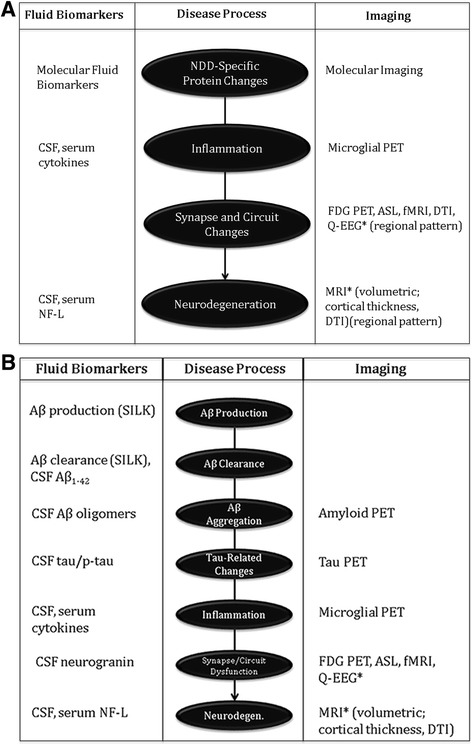
Discussion: Defining disease-modification is critical to drug-development programs. A DMT is an intervention that produces an enduring change in the trajectory of clinical decline of an NDD by impacting the disease processes leading to nerve cell death. A DMT is neuroprotective, and neuroprotection will result in disease modification. Disease modification can be demonstrated in clinical trials by a drug-placebo difference in clinical outcomes supported by a drug-placebo difference on biomarkers reflective of the fundamental pathophysiology of the NDD. Alternatively, disease modification can be supported by findings on a staggered start or delayed withdrawal clinical trial design. Collecting multiple biomarkers is necessary to support a comprehensive view of disease modification.
Conclusion: Disease modification is established by demonstrating an enduring change in the clinical trajectory of an NDD based on intervention in the fundamental pathophysiology of the disease leading to nerve cell death. Supporting data are collected in clinical trials. Effectively defining a DMT will assist in NDD drug development programs.
Keywords: Alzheimer’s disease; Amyotropic lateral sclerosis; Corticobasal degeneration; Disease modification; Disease modifying therapy; Frontotemporal dementia; Multiple system atrophy; Progressive supranuclear palsy.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
JC has provided consultation to Abbvie, Acadia, Actinogen, Alzheon, Anavex, Avanir, Axovant, Boehinger-Ingelheim, Bracket, Eisai, Forum, GE Healthcare, Genentech, Intracellular Interventions, Lilly, Lundbeck, Medavante, Merck, Neurocog, Novartis, Orion, Otsuka, Pfizer, Piramal, QR, Roche, Suven, Sunovion, Takeda and Toyama pharmaceutical and assessment companies.
Figures

References
-
- Coupe C, Gordon PH. Amyotrophic lateral sclerosis - clinical features, pathophysiology and management. European Neurol Rev. 2013;8:38–44. doi: 10.17925/ENR.2013.08.01.38. - DOI
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
